Session Information
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: Q fever, an endemic disease in Southern California, is a zoonosis caused by Coxiella burnetii. The infection can present with multiple non-specific acute and chronic manifestations including fever, headache, fatigue, endocarditis, and hepatitis. Q fever is also associated with the presence of elevated inflammatory markers and autoimmune antibodies. This combination of the clinical picture and laboratory features may be misinterpreted for various rheumatologic conditions.
Methods: We evaluated records of patients who were newly diagnosed with Q-fever during an inpatient stay at 2 academic medical centers from 2013 to 2021. Data was collected for all Q fever cases in whom rheumatology was consulted, including demographics, symptoms on admission, comorbidities, labs, imaging, tissue sample obtained, and medical specialties consulted. Inpatient rheumatology consultation reports were reviewed. The reason for the consult, differential diagnosis, the time it took from admission to rheumatology consult, and rheumatology consult to Q fever diagnosis were analyzed.
Results: From 2013-2021, 23 patients were diagnosed with Q fever during an inpatient stay. Eight patients (34.7%) received rheumatology consultation prior to their Q fever diagnosis. Majority of the patients (62.5%) had symptom onset during the first quarter of the year, 75% of patients had exposure to cattle, sheep, goat, or rats, 37.5% had domestic pet exposure, and 1 patient did not report any known animal exposure. Almost all (87.5%) patients had fever and flu-like symptoms, with 63% having GI symptoms. All patients had extensive infectious workup done. All patients had elevated inflammatory markers, and 63% with abnormal liver enzymes. One patient had a low titer antinuclear antibody and another one had a positive rheumatoid factor. Two patients underwent liver biopsy showing ring granulomas and granulomatous hepatitis, findings characteristic but not pathognomonic of Q fever.
Fever of unknown origin (FUO) was the most common (75%) reason for consultation while one patient each was referred for evaluation for giant cell arteritis (GCA) and sarcoidosis. In 50% of cases, the rheumatology service thought a rheumatologic disease is less likely and thus recommended additional studies for infectious or oncologic etiology. Rheumatologic differentials included adult-onset Still’s disease, Bechet’s disease, sarcoidosis, and systemic vasculitis including GCA. An auto-inflammatory gene panel was done in 2 patients and temporal artery biopsy was done in 1 patient with results all negative. On average, Q fever was diagnosed approximately 10.6 days after admission and 5.8 days after rheumatology consultation.
Conclusion: The non-specific presentation of Q fever, accompanied by elevated inflammatory markers, and autoimmune antibodies can mimic various rheumatologic conditions including vasculitis, Still’s disease, and sarcoidosis. Our case series demonstrates that Q-fever should be considered as a differential diagnosis especially for patients with FUO and residing in endemic regions.
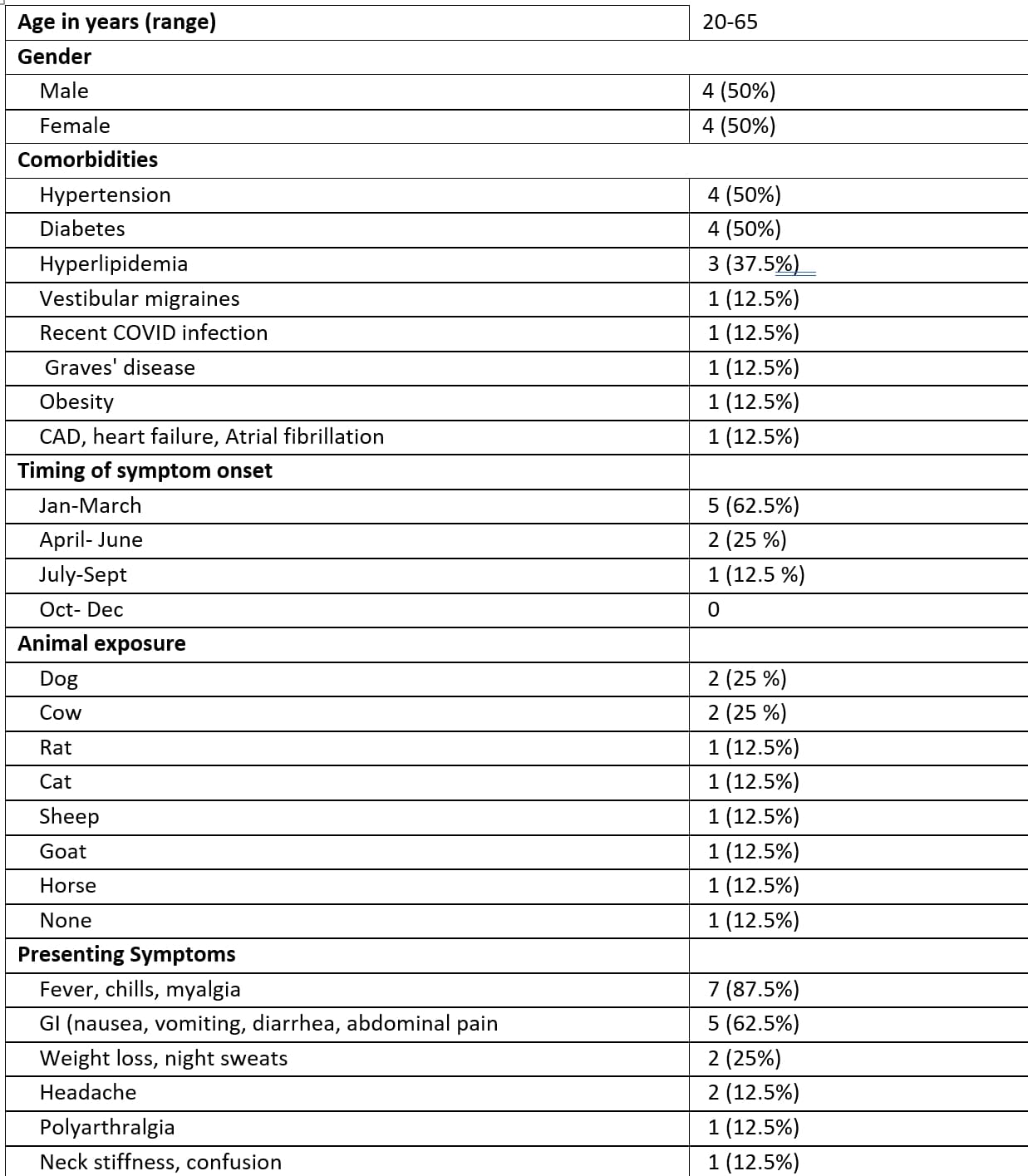 Table 1. Patient demographics and presenting symptoms of patients diagnosed with Q fever patients who received Rheumatology inpatient consultation (n=8)
Table 1. Patient demographics and presenting symptoms of patients diagnosed with Q fever patients who received Rheumatology inpatient consultation (n=8)
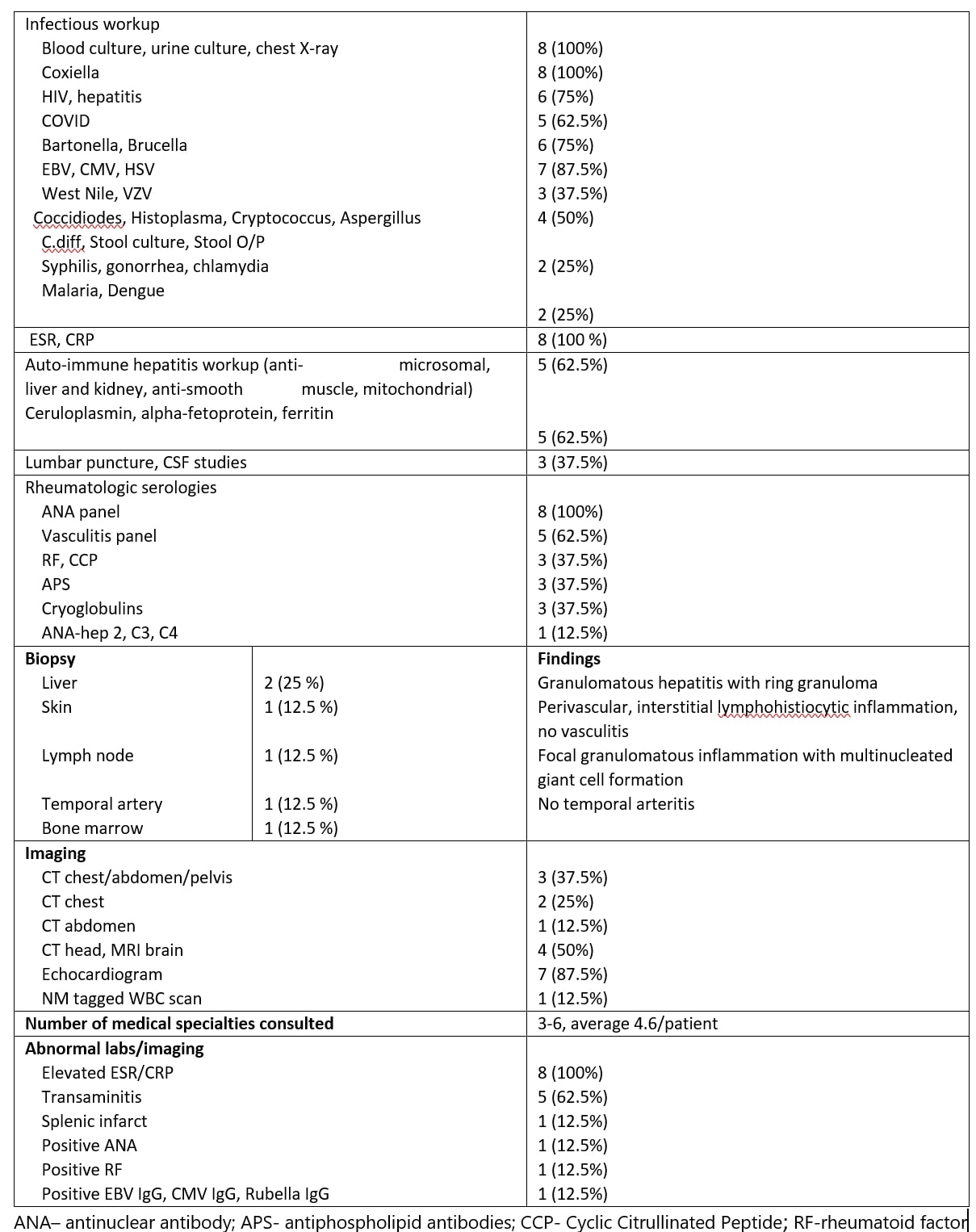 Table 2. Work-up done prior to rheumatology consult, specialties consulted, and abnormal results
Table 2. Work-up done prior to rheumatology consult, specialties consulted, and abnormal results
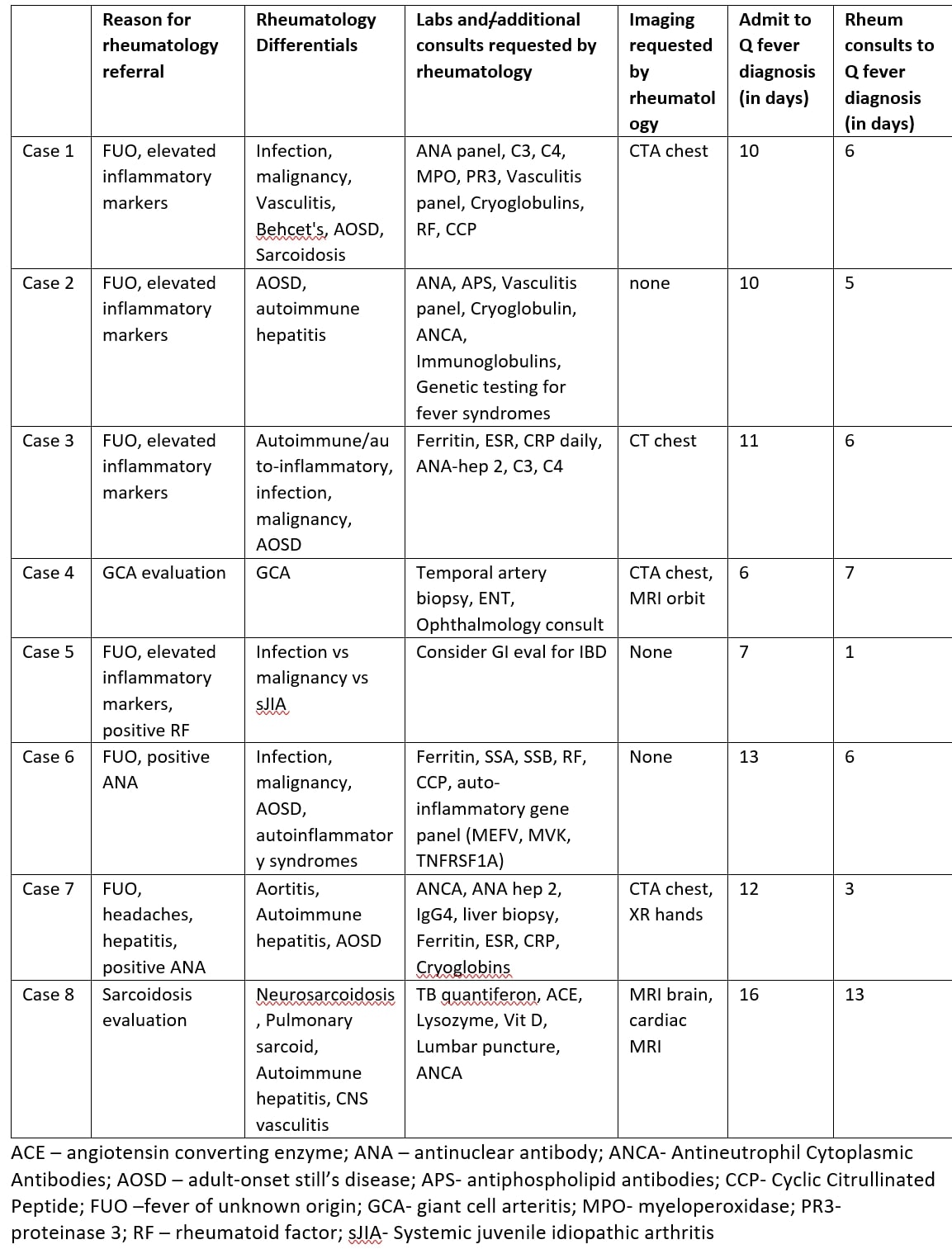 Table 3. Details on rheumatology consultation, differentials, and workup
Table 3. Details on rheumatology consultation, differentials, and workup
To cite this abstract in AMA style:
Aggarwal M, Cabling M. Q Fever as a Mimicker of Rheumatologic Conditions: A Case Series from Two Tertiary Care Academic Centers in Southern California [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/q-fever-as-a-mimicker-of-rheumatologic-conditions-a-case-series-from-two-tertiary-care-academic-centers-in-southern-california/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/q-fever-as-a-mimicker-of-rheumatologic-conditions-a-case-series-from-two-tertiary-care-academic-centers-in-southern-california/