Session Information
Session Type: Abstract Session
Session Time: 12:45PM-1:00PM
Background/Purpose: Idiopathic inflammatory myopathies (IIM) are a group of diseases characterized by muscular and systemic involvement, with interstitial lung disease (ILD) being a challenging problem. High-resolution tomography (HRCT) is the current reference standard for diagnosing ILD; however, there are limitations related to its cost, accessibility, and the use of ionizing radiation. Lung ultrasound (LUS) has recently been used to detect ILD associated with other rheumatic diseases, which may justify its use as a screening method for clinical suspicion of ILD. However, evidence on using LUS in ILD associated with IIM is limited. We aimed to characterize the LUS findings in patients with IIM and their relationship with clinical features and antibodies.
Methods: Patients diagnosed with IIM according to the ACR/EULAR 2017 Classification Criteria were included, and they underwent HRCT, LUS, and pulmonary function tests (PFT). The Warrick score was used to assess the severity and extent of ILD. Ultrasound was performed using a LOGIQTMe device with a 4-12 MHz linear probe, applying two scanning methods (14 predetermined intercostal space (ICS) and 12 posterior-basal ICS). “B” lines (BL) and pleural abnormalities (PA) were documented for each ICS. Descriptive statistics were used based on the distribution of the variables, ROC curve analysis was conducted, and the sensitivity and specificity of LUS for detecting ILD compared to HRCT were calculated. Correlations were analyzed using the Spearman correlation coefficient between the ultrasound findings, the Warrick score, and the PFT.
Results: We included 59 patients diagnosed with IIM, mostly women (79.7%). The median and interquartile range (IQR) of age enrolment was 52 years (39.0-60.5). The most common diagnoses were dermatomyositis (72.9%) and antisynthetase syndrome (15.3%). The most frequent antibodies in the recruited patients were Ro-52 (30.5%), Mi-2 (23.7%), and MDA-5 (16.9%). The prevalence of ILD was 64.4%. Relevant baseline characteristics are shown in Table 1.A positive, strong correlation was demonstrated between the Warrick score and B-line count in 14 ICS (rho= 0.64, p< 0.0001) and 12 ICS (rho=0.54, p< 0.0001). Also, a positive correlation was observed between pleural line abnormalities and the Warrick score (rho=0.59,p< 0.0001). Table 2.The AUCs were 0.95 (95% CI, 0.88-1.00), 0.85 (95% CI, 0.74-0.96), and 0.91 (95% CI, 0.82-0.99) for the evaluation of the number of B-lines in 14 ICS, 12 ICS, and the number of ICS with pleural abnormalities (22 EIC), respectively. Image 1
Conclusion: Our study confirms that LUS is a valuable tool for detecting ILD in patients with IIM. It offers real-time visualization and high diagnostic accuracy by quantifying B-lines and evaluating pleural abnormalities using either of the two scanning protocols (14 and 12 ICS). The method demonstrates strong diagnostic performance and a good correlation with the Warrick scores.
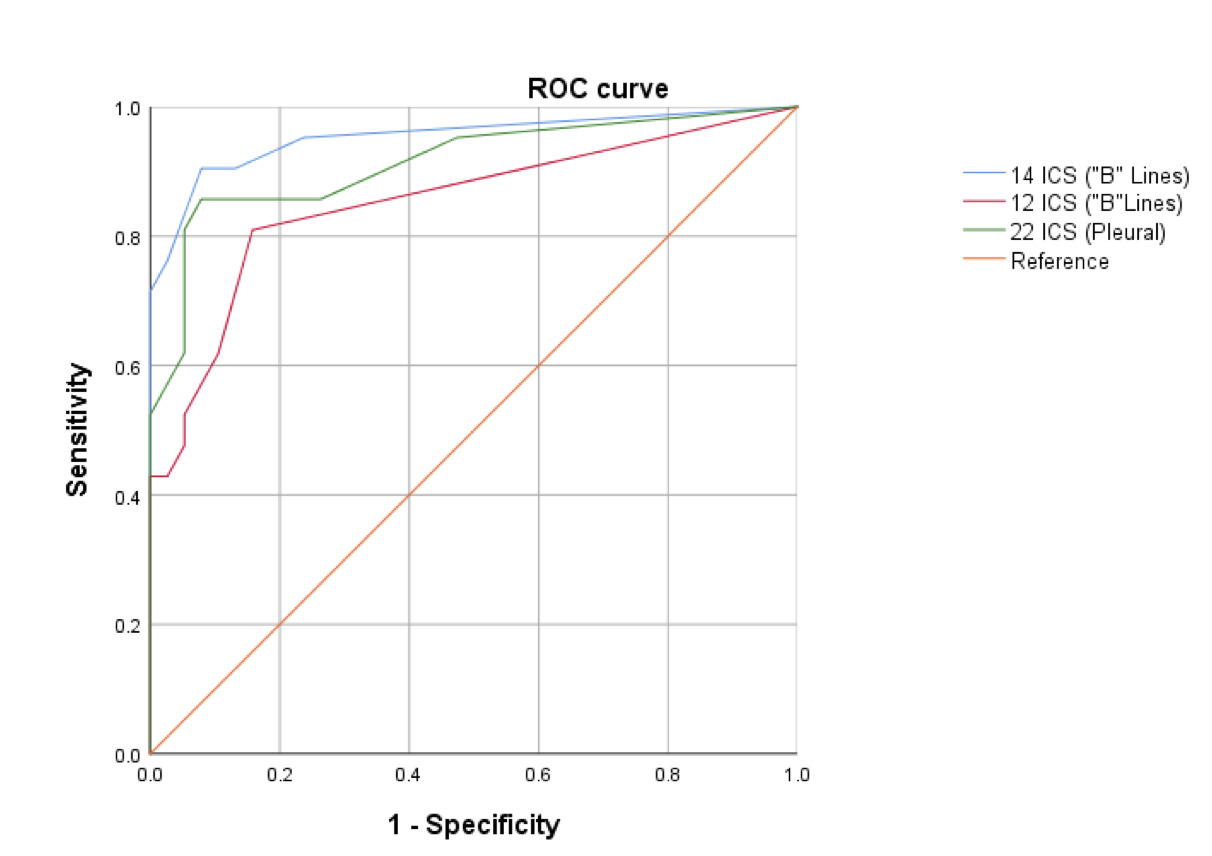 Table 1. General Characteristics
Table 1. General Characteristics
.jpg) Table 2. Correlations between ultrasonographic findings and Warrick score
Table 2. Correlations between ultrasonographic findings and Warrick score
.jpg) Image 1. ROC curve of ultrasonographic findings
Image 1. ROC curve of ultrasonographic findings
To cite this abstract in AMA style:
Mora A, Soto-Fajardo C, Torres-Ruiz J, Gómez-Martín D, Carranza F, Cano T, Cervantes Ramírez E, Espinosa A, Reyna Juárez Y, Pineda C. Pulmonary ultrasound findings and their relationship with clinical characteristics and myopathy antibodies in a cohort of patients with myositis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/pulmonary-ultrasound-findings-and-their-relationship-with-clinical-characteristics-and-myopathy-antibodies-in-a-cohort-of-patients-with-myositis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pulmonary-ultrasound-findings-and-their-relationship-with-clinical-characteristics-and-myopathy-antibodies-in-a-cohort-of-patients-with-myositis/