Session Information
Session Type: Poster Session B
Session Time: 5:00PM-6:00PM
Background/Purpose: Patients with JDM are at increased risk of infection due to increased aspiration risk and immunosuppression. Procalcitonin (PCT) is a biomarker of infection, that has a growing role in both diagnosis of bacterial infection and antibiotic management. PCT rises in response to bacterial infections such as pneumonia or sepsis; however, studies have shown that PCT is also elevated in sJIA, MAS or SLE even in the absence of infection. The objectives of this study were to investigate whether PCT is elevated in patients with active JDM and if PCT correlates with JDM disease activity. If PCT is not associated with JDM activity, it may remain a reasonable choice to screen for bacterial infection. If PCT is associated with JDM activity, it may serve as a tool to monitor JDM activity; however, its utility for bacterial infection detection would be reduced.
Methods: Data and serum samples were obtained from the Cure JM biorepository and registry. Control samples were obtained from previously stored samples (housed in the biorepository) of allergy clinic patients under 18 years of age with non-allergic rhinitis. Inclusion criteria for the JDM samples included a diagnosis of JDM by the Bohan and Peter criteria and availability of clinical data and a serum sample within 4 months of enrollment. Exclusion criteria were age greater than 18 years. PCT concentration of the serum samples was determined by the central clinical laboratory through electrochemiluminescence. Laboratory (muscle enzymes, MSAs, NK cells, inflammatory markers) and clinical characteristics (demographics, Childhood Myositis Assessment Scale (CMAS), Disease Activity Scores) for the JDM patients were obtained from the registry from the closest collection point to serum acquisition. A Fishers exact test was used to compare the proportions of JDM and control groups with PCT levels above and below the detection threshold of 0.1. Spearman correlation was used to assess the correlation between PCT values and markers of JDM disease activity among patients with detectable PCT levels.
Results: We obtained the serum of 44 patients with recently diagnosed JDM along with 21 sex-matched healthy controls. Of the 44 JDM patients, 6 patients had a detectable PCT levels with the highest PCT value obtained being 0.39 ng/ml. All of the controls had undetectable PCT levels. The proportion of patients with detectable PCT levels was not significantly elevated in JDM compared to controls (p= 0.17). Among the 6 patients with abnormal PCT, there was no correlation between PCT level and other markers of JDM disease activity.
Conclusion: The proportion of children with detectable PCT levels was not significantly higher among those with JDM compared to controls, suggesting that elevated PCT levels are not a marker of JDM. This study suggests that moderately or highly elevated PCT levels in JDM patients are unlikely to be due to their autoimmune disease. PCT did not correlate with typical markers of JDM disease activity although this analysis was limited due to the small number of JDM patients with abnormal PCT. Further studies including a higher proportion of JDM patients with elevated PCT are needed to explore potential associations that may not have been captured in this study.
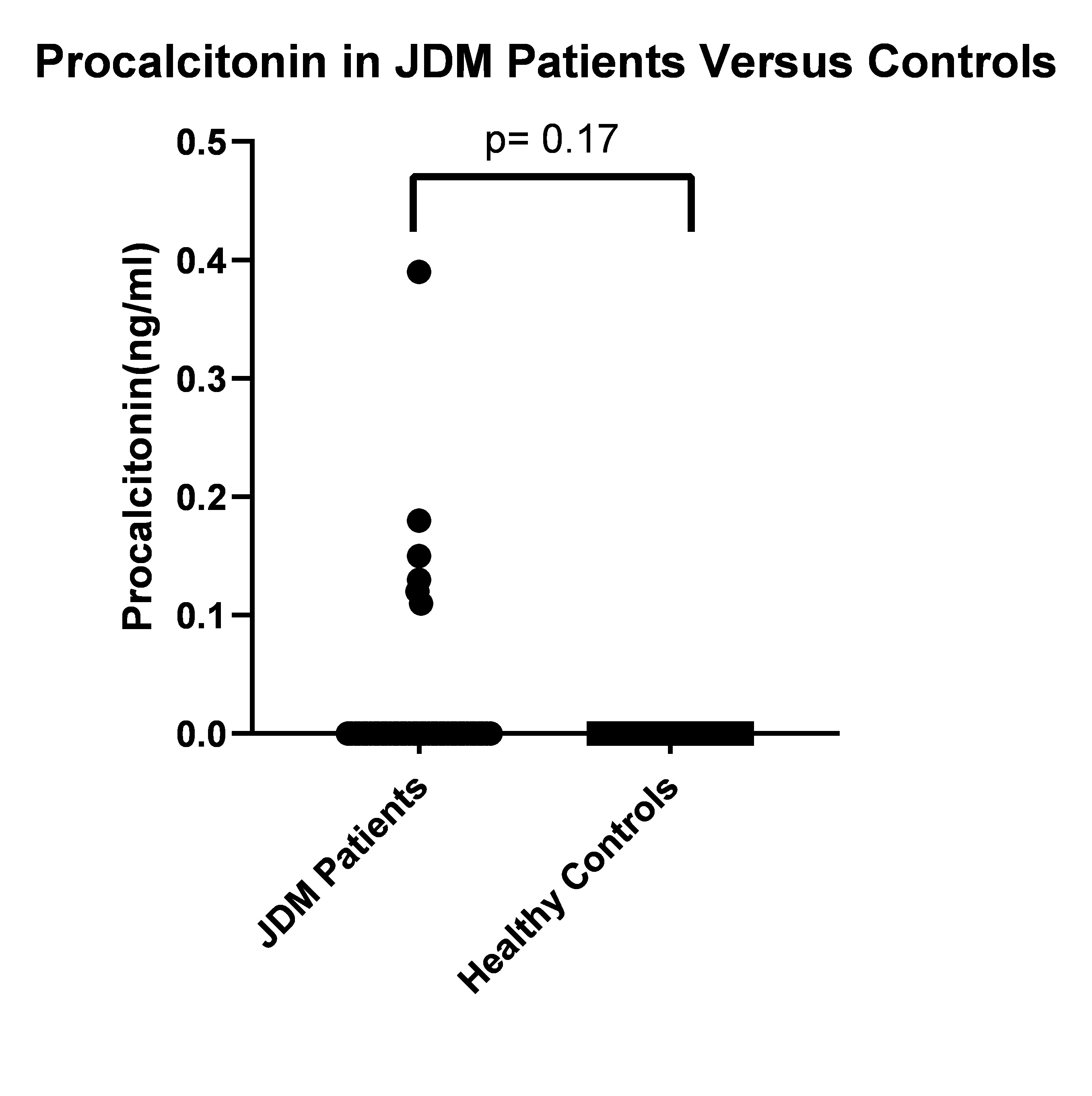 Figure 1: Box Plot Comparing PCT levels by Fisher Exact Test Between JDM Patients and Healthy Controls
Figure 1: Box Plot Comparing PCT levels by Fisher Exact Test Between JDM Patients and Healthy Controls

To cite this abstract in AMA style:
Costin C, Morgan G, Muhammad L, Khojah A, Klein-Gitelman M, Lee Y, Pachman L. Procalcitonin Levels in Patients with Juvenile Dermatomyositis Compared to Healthy Controls [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 4). https://acrabstracts.org/abstract/procalcitonin-levels-in-patients-with-juvenile-dermatomyositis-compared-to-healthy-controls/. Accessed .« Back to 2023 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/procalcitonin-levels-in-patients-with-juvenile-dermatomyositis-compared-to-healthy-controls/