Session Information
Date: Monday, November 14, 2022
Title: Abstracts: RA – Diagnosis, Manifestations, and Outcomes III: RA ILD
Session Type: Abstract Session
Session Time: 4:30PM-6:00PM
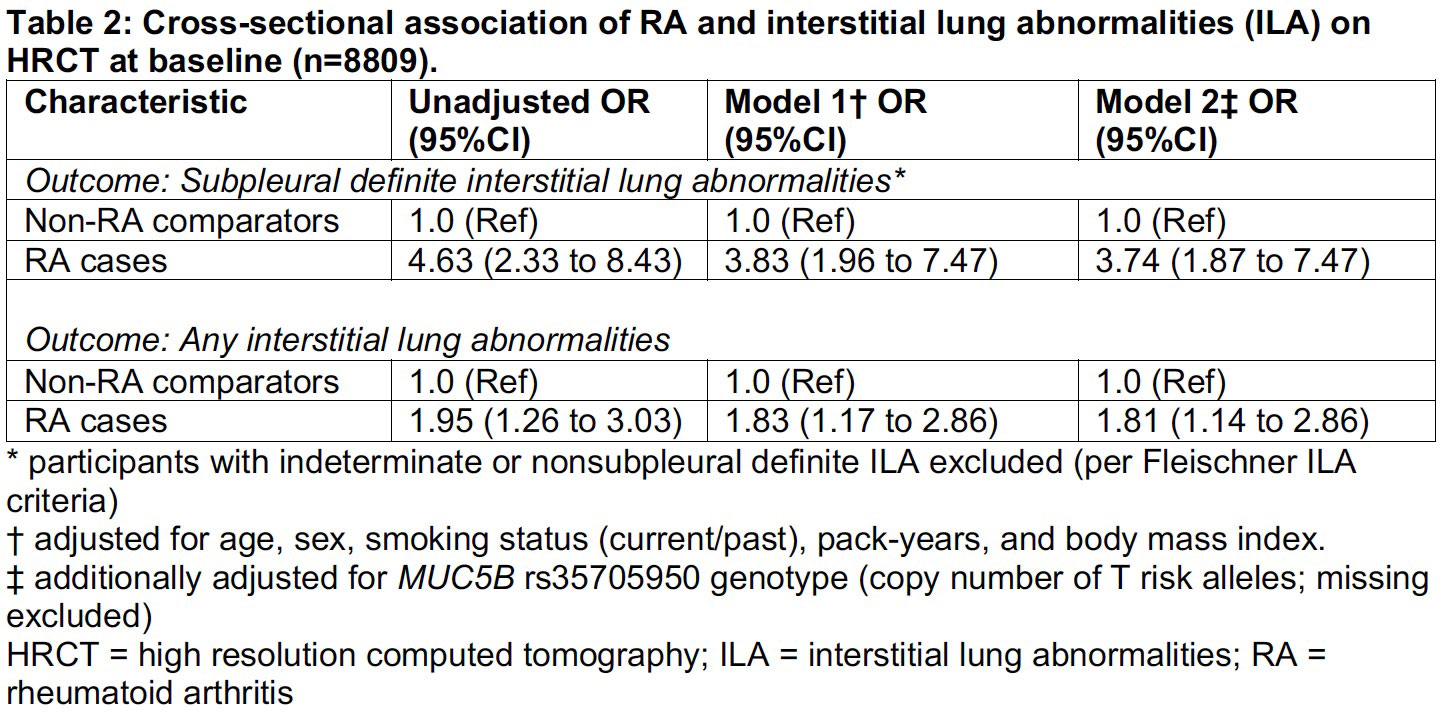
Background/Purpose: Subpleural interstitial lung abnormalities (ILA) may be a form of subclinical or preclinical interstitial lung disease (ILD) and have been reported in up to a third of RA patients in screening studies. However, few studies screened for ILA in a sample that included RA cases and non-RA comparators, and none investigated long-term mortality after detection of RA with ILA. Therefore, we performed a case-control study examining the cross-sectional prevalence of RA with ILA and a cohort study of the long-term mortality risk of ILA in participants with and without RA.
Methods: We investigated the association of RA with ILA and long-term mortality risk in COPDGene, a multicenter prospective cohort of current or former smokers with at least 10 pack-years of smoking history. Patients with known ILD or bronchiectasis were excluded. Baseline visits occurred between 2007-2012 and included high-resolution chest CT (HRCT), whole genome sequencing (including the MUC5B promoter variant, the strongest genetic RA-ILD risk factor), and surveys. We identified prevalent RA cases by self-report of RA and DMARD use (PPV 88%). Comparators reported no RA or DMARD use. ILA were identified by a sequential reader review of HRCT images by up to 3 expert readers to classify ILA as present, indeterminate, or absent. ILA was defined as nondependent subpleural or non-subpleural interstitial changes affecting >5% of any lobar area. Indeterminate ILA was focal or unilateral changes, or patchy groundglass opacities affecting < 5% of a lobar region. Death was ascertained through longitudinal study follow up and periodic searches of the social security death index. We examined the association of RA case vs comparator status with ILA using multivariable logistic regression. In the cohort study, we investigated RA and ILA mortality risk using multivariable Cox regression, adjusted for potential confounders.
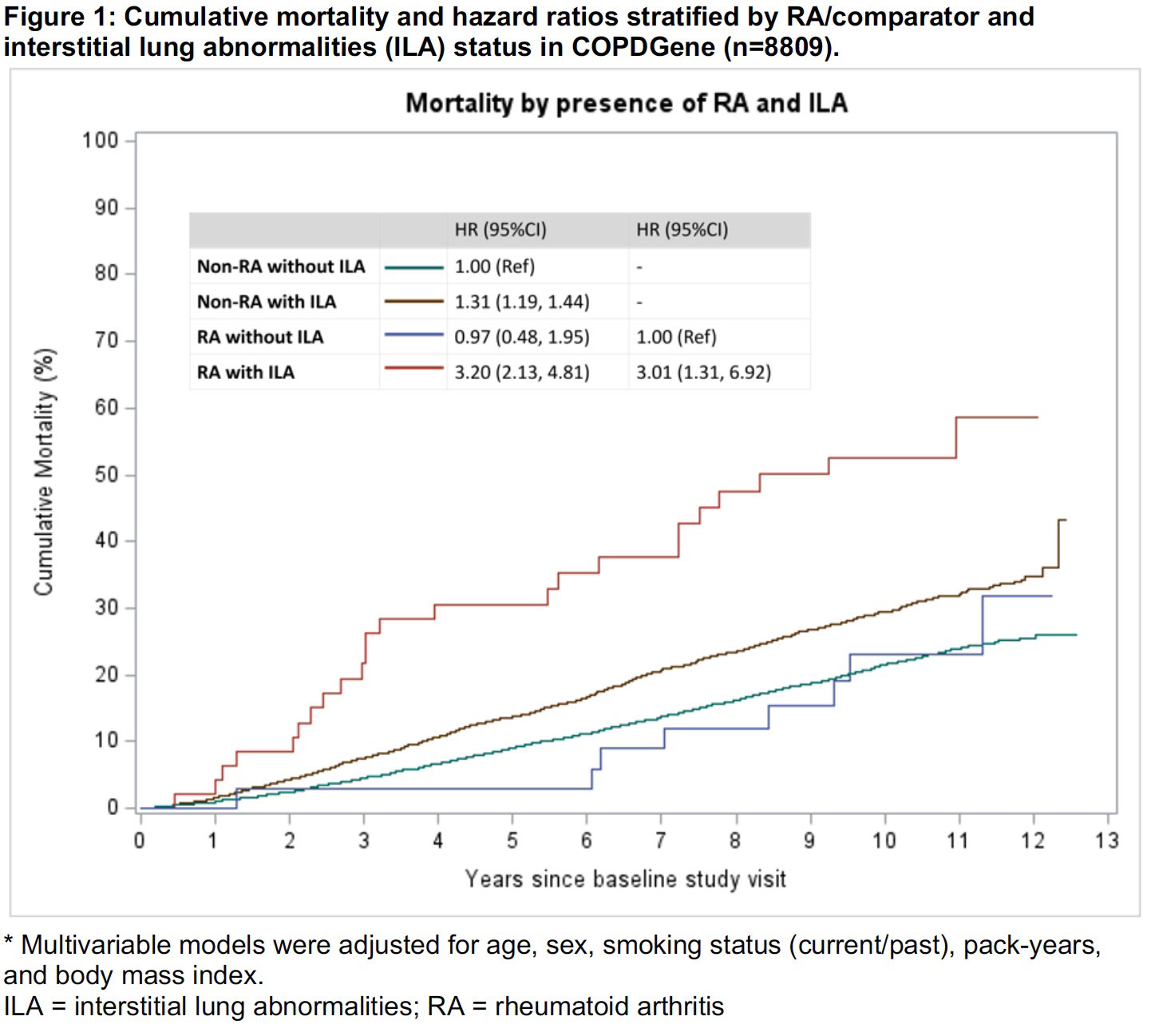
Results: We analyzed 82 RA cases and 8727 non-RA comparators with HRCT performed for research purposes. The prevalence of subpleural ILA was 15.9% in RA cases compared to 5.0% in non-RA comparators. Compared to non-RA, RA had OR 3.74 (95%CI 1.87 to 7.47) for subpleural ILA after adjustment for age, sex, BMI, smoking status, pack-years, BMI, and MUC5B promoter status. During median follow up of 9.4 years, there were 1852 (21%) deaths. The 10-year mortality for RA cases with ILA or indeterminate ILA was 53% (95%CI 39 to 68%) compared to 23% (95%CI 12 to 43%) and 22% (95%CI 20 to 23%) for RA without ILA and non-RA without ILA, respectively (log-rank p< 0.0001). RA with ILA was strongly associated with mortality compared to non-RA without ILA (multivariable HR 3.20 95%CI 2.13 to 4.81). Among only RA cases, RA with ILA was associated with increased mortality compared to RA without ILA (multivariable HR 3.01, 95%CI 1.31 to 6.92).
Conclusion: We confirmed that RA was strongly associated with ILA in this large comparative study, and this finding persisted after adjustment for smoking intensity/duration and the MUC5B promoter variant. RA patients with ILA had 3-fold increased mortality, emphasizing an urgent need for research to determine the possible clinical utility of screening, monitoring, and early treatment of subclinical ILD.

To cite this abstract in AMA style:
McDermott G, Hayashi K, Yoshida K, Moll M, Cho M, Doyle T, Dellaripa P, Putman R, San Jose Estepar R, Washko G, Regan E, Hatabu H, Hunninghake G, Silverman E, Sparks J. Prevalence and Mortality of Interstitial Lung Abnormalities in Rheumatoid Arthritis and non-RA Comparators in a Multicenter Prospective Cohort [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/prevalence-and-mortality-of-interstitial-lung-abnormalities-in-rheumatoid-arthritis-and-non-ra-comparators-in-a-multicenter-prospective-cohort/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/prevalence-and-mortality-of-interstitial-lung-abnormalities-in-rheumatoid-arthritis-and-non-ra-comparators-in-a-multicenter-prospective-cohort/