Session Information
Date: Monday, November 18, 2024
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Giant cell arteritis (GCA) is a vasculitis affecting individuals aged ≥50 years. Over 80% of patients with GCA are aged ≥70 years, reflecting a significant disease burden among people covered by the United States Medicare program. The objective of this study was to assess the prevalence and incidence of GCA in the United States Medicare fee-for-service (FFS) population and evaluate variations in the epidemiology of GCA based on age, sex, and race/ethnicity.
Methods: This retrospective observational cohort study was based on the most recently available Research Identifiable Files from the Centers for Medicare and Medicaid Services (CMS). The study included Medicare FFS beneficiaries eligible by age ≥65 years with ≥1 inpatient or ≥2 outpatient claims with a GCA diagnosis code 7+ days apart but within 365 days. For incidence estimates, the diagnosis of GCA had to occur within the calendar year of interest with no GCA diagnosis in the calendar year prior. Temporal artery biopsy within 60 days of the index GCA diagnosis date was required for all incident (new onset) patients. Continuous enrollment (without a Medicare Advantage plan) was required in the calendar year of interest for prevalence analyses, and for both the current and prior years for incidence analyses. Prevalence and incidence rates were calculated from 2014 to 2019, the 5 most recent years preceding the COVID-19 pandemic, and stratified by age, sex, and race/ethnicity in 2019.
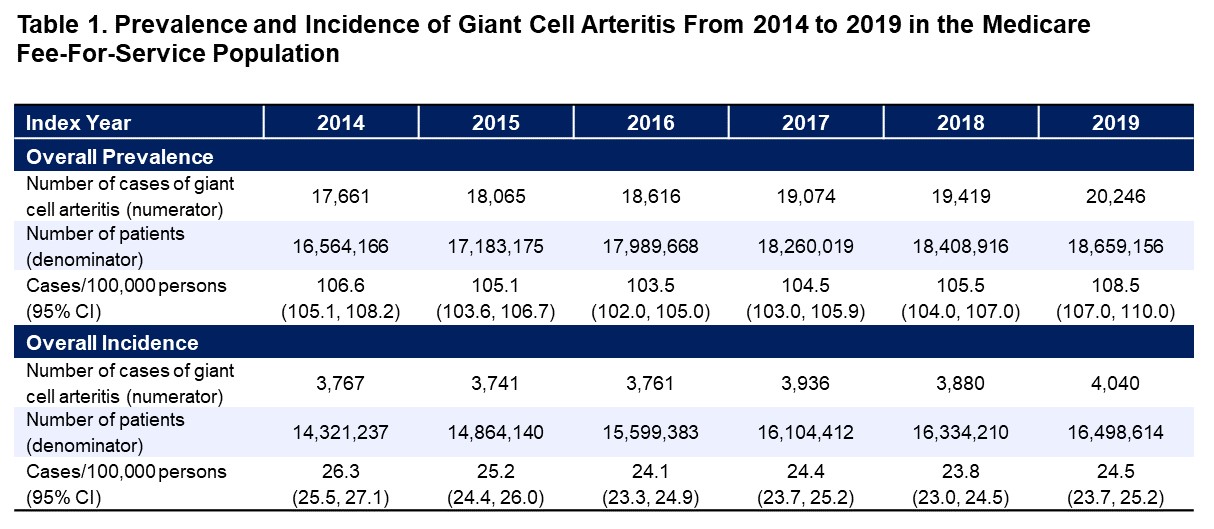
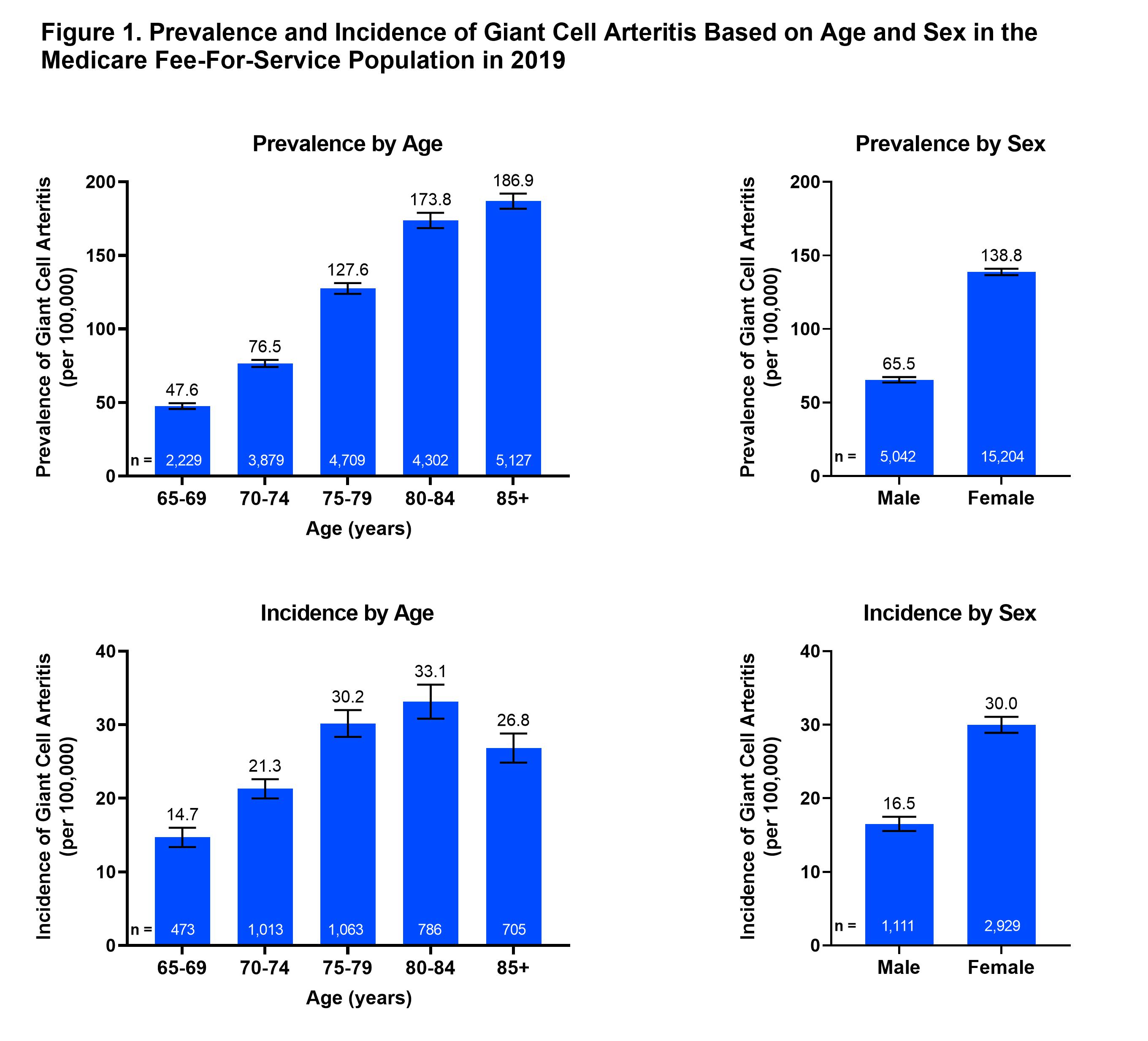
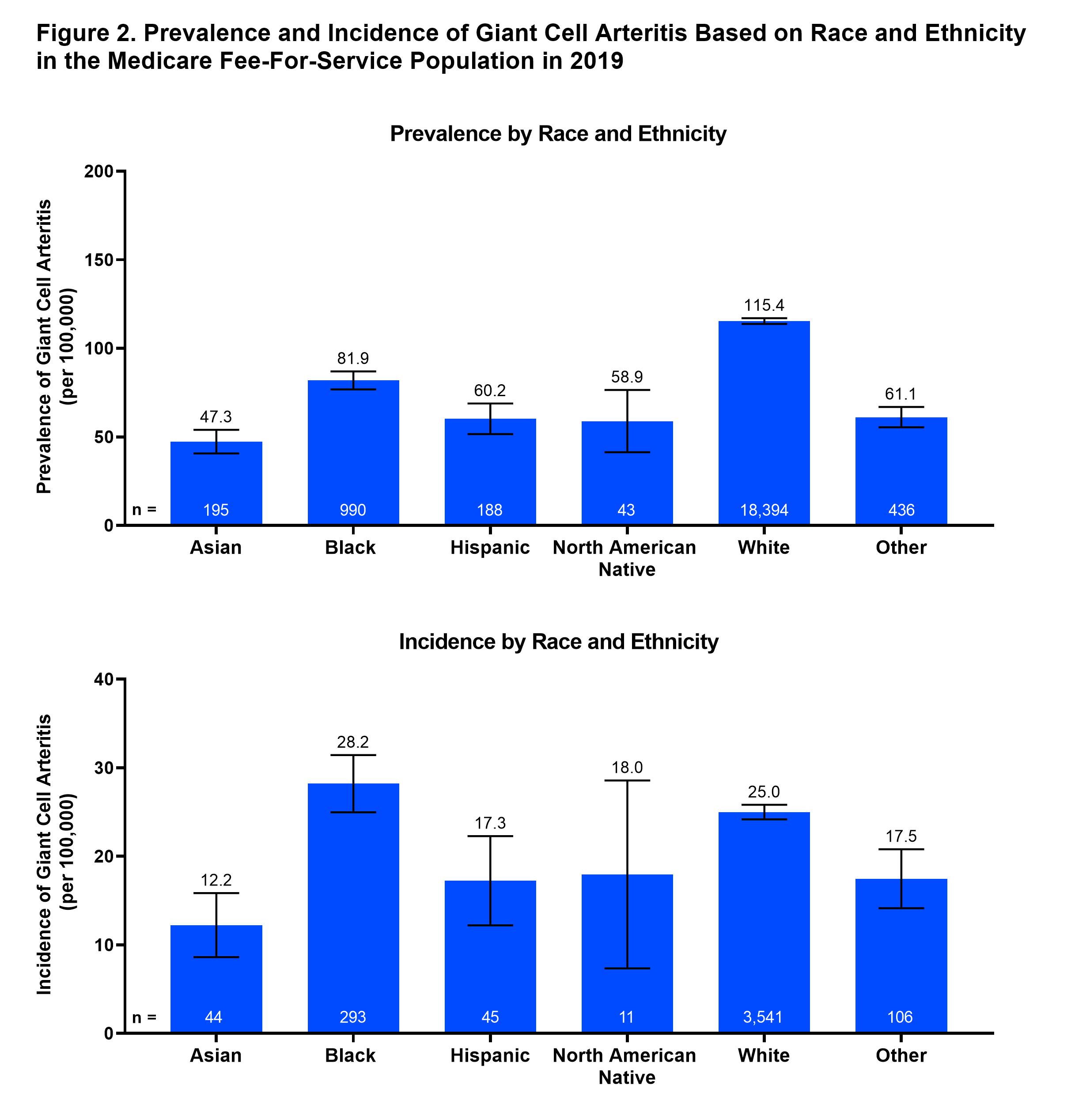
Results: In the Medicare FFS population, which represents ~67% of all Medicare enrollees from 2014 to 2019, the rates of a diagnosis of GCA remained stable during the study period. The annual prevalence ranged from 103.5 to 108.5 cases/100,000 persons, while the incidence ranged from 23.8 to 26.3 cases/100,000 persons (Table 1). The prevalence of GCA increased with age, with patients over 85+ years having a prevalence rate nearly 4-times higher than those aged 65 to 69 years (186.9 vs 47.6 cases/100,000 persons in 2019) (Figure 1). Similarly, the incidence of GCA also increased with age, with the highest rate observed in the 80 to 84-year age group. Prevalence and incidence of GCA were approximately twice as high in females than males. Prevalence of GCA was highest in White persons compared to other race/ethnicity subgroups; among non-White persons, rates were highest among Black persons and lowest in Asian persons (Figure 2). Incidence estimates by race/ethnicity were difficult to interpret given small sample sizes among non-White persons.
Conclusion: Among United States Medicare FFS patients, the average annual prevalence and incidence rates of GCA were 105.6 and 24.7 cases/100,000 persons, respectively; these rates were stable during the 5-year study period. GCA was twice as common in females than in males and increased with age for both sexes. The prevalence of GCA varied substantially by race: highest in White persons, lowest rates in Asian persons. A limitation of these results is the exclusion of patients aged 50 to 65 years and non-FFS Medicare populations. By leveraging the largest available national population database, characterized by continuous coverage, this analysis provides strong data on the epidemiology of GCA in the United States.
To cite this abstract in AMA style:
Merkel P, Peng Y, Zueger P, Ziadeh C, Romero A, Thielen R, Kruzikas D. Prevalence and Incidence of Giant Cell Arteritis Among Medicare Fee-For-Service Beneficiaries: United States, 2014–2019 [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/prevalence-and-incidence-of-giant-cell-arteritis-among-medicare-fee-for-service-beneficiaries-united-states-2014-2019/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/prevalence-and-incidence-of-giant-cell-arteritis-among-medicare-fee-for-service-beneficiaries-united-states-2014-2019/