Session Information
Date: Sunday, October 26, 2025
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Concomitant fibromyalgia (FM) can be suspected in patients (pts) with axial SpA (axSpA) using the Fibromyalgia Rapid Screening Tool (FiRST).The objective of this study was to evaluate the prevalence of suspected FM and its impact on the disease, including first TNFi initiation and retention rates, PROs and disability, over the first 10 years of follow-up in pts with axSpA.
Methods: This analysis included pts diagnosed with axSpA by a rheumatologist for less than 3 years. Collected data: The FiRST tool became available starting from the seventh year (M84) and was then administered annually until year 10 (M120). Statistical analysis: a) Estimation of FM prevalence. The percentage of FM+ pts was estimated for the entire cohort (n=708). Missing data were imputed using multiple imputation for longitudinal data at each of the four visits (M84 to M120). A patient was classified as FM+ if he/she was identified as FiRST+ at least twice during the four visits (M84-M120) after multiple imputation. b) Impact of FM: The impact of FM was assessed as follows: b.1.) at the start of the cohort (visit M0): by comparing objective signs of axSpA (HLA-B27 status, structural damage on X-rays, inflammation on MRI-SIJ and abnormal CRP); b.2.) over the 10 years of follow-up: by analysing disease activity, PROs and disability using mixed models for repeated measures; b.3.) therapeutic impact: by evaluating the percentage of patients treated with a first TNFi and their therapeutic maintenance using Kaplan-Meier analyses.
Results: After the multiple imputation of visits M84 to M120, the estimated prevalence of FM+ pts was 144/663 (21.7%). At baseline, the presence of FM was associated with a lower frequency of HLA-B27 positivity and radiographic sacroiliitis, but a similar prevalence of positive MRI-SIJ findings and abnormal CRP levels. Furthermore, the level of confidence in the SpA diagnosis by the rheumatologist was similar in FM+ and FM- groups (6.9 vs. 7.1 on a 0-10 scale).The presence of FM was also associated with higher disease activity and poorer quality of life over the 10 years of follow up (Figure 1). Pts with FM showed a significant greater likelihood of reporting permanent disability after 10 years compared to FM- pts (26.4% vs. 9.4%, p< 0.001). Finally, FM+ was associated with a higher likelihood of initiating biologic therapy during the 10 years of follow-up (64.4% vs. 46.1%). However, therapeutic maintenance was poorer in the FM+ group, with a lower percentage of pts remaining on treatment one year after initiation [FM+: 42.0% (95%CI 32.1-54.9) vs. FM-: 64.2% (95%CI 57.9-71.2)] (Figure 2).
Conclusion: This study confirms the high prevalence of FM in axSpA. The similarity of certain objective disease markers (e.g., MRI-SIJ positivity and abnormal CRP) between FM+ vs. FM- pts, as well as the comparable diagnostic confidence, suggests that FM is more likely a comorbidity than a diagnostic error. The presence of FM negatively impacts disease activity scores and quality of life, resulting in a higher likelihood of permanent disability. FM is also associated with an increased likelihood of initiating biologic therapy; however, therapeutic maintenance is lower in these pts.
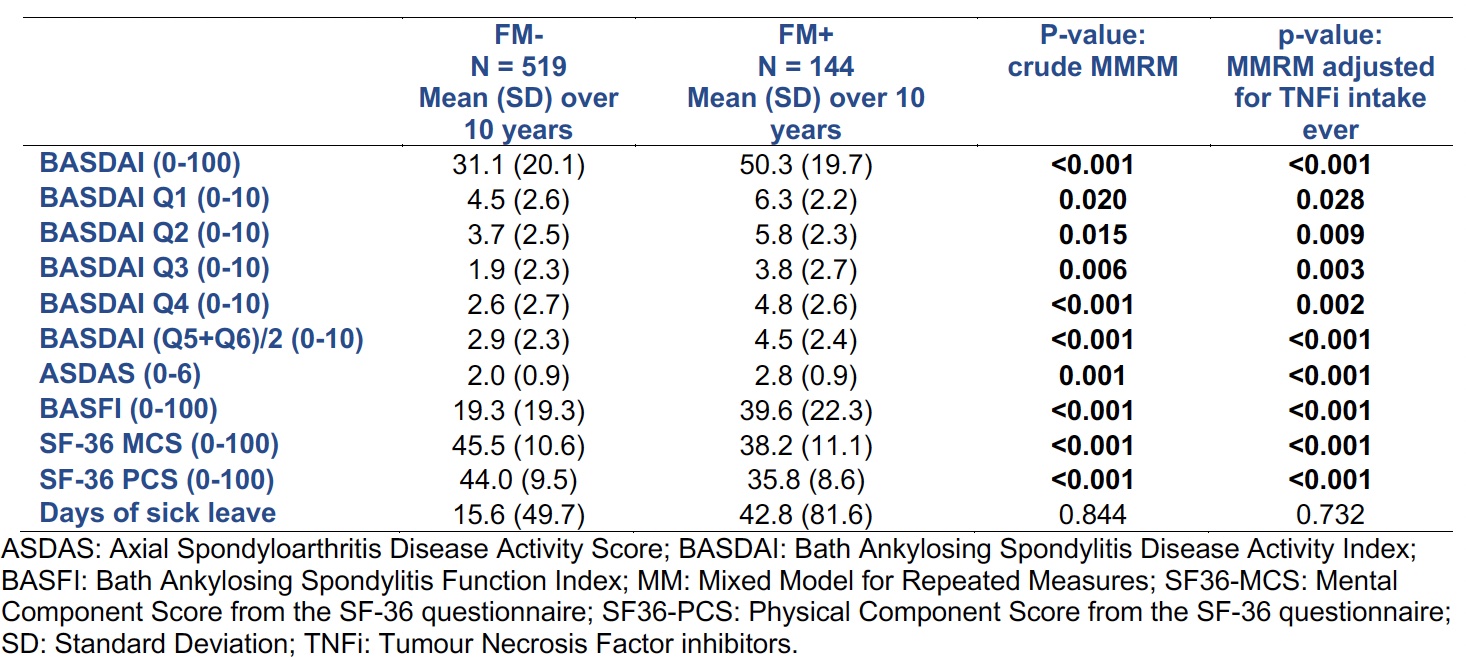 Figure 1. Mixed models for Repeated Measures (MMRM) with random effects to compare disease activity and PROs over 10 years of follow-up between FM+ and FM-.
Figure 1. Mixed models for Repeated Measures (MMRM) with random effects to compare disease activity and PROs over 10 years of follow-up between FM+ and FM-.
.jpg) Figure 2. Impact of concomitant FM on the probability of TNFi initiation (A) and on the retention rate to the first TNFi (B).
Figure 2. Impact of concomitant FM on the probability of TNFi initiation (A) and on the retention rate to the first TNFi (B).
To cite this abstract in AMA style:
López Medina C, Chevret S, Lukas C, Molto A, Dougados M. Prevalence and Impact of Fibromyalgia on Disease Outcomes and Treatment in Axial Spondyloarthritis: 10-year Follow-up Data From the DESIR Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/prevalence-and-impact-of-fibromyalgia-on-disease-outcomes-and-treatment-in-axial-spondyloarthritis-10-year-follow-up-data-from-the-desir-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/prevalence-and-impact-of-fibromyalgia-on-disease-outcomes-and-treatment-in-axial-spondyloarthritis-10-year-follow-up-data-from-the-desir-cohort/