Session Information
Date: Monday, November 9, 2020
Session Type: Abstract Session
Session Time: 5:00PM-5:50PM
Background/Purpose: There is lack of international consensus as to what defines a structural lesion on MRI of the sacroiliac joints (SIJ) typical of axial spondyloarthritis (axSpA). The ASAS MRI group has generated updated consensus lesion definitions that describe each of the MRI lesions in the SIJ1 which have been validated by 8 readers from the ASAS-MRI group on MRI images from the ASAS Classification Cohort2,3. We aimed to identify quantitative cut-offs based on numbers of slices and SIJ quadrants that define a positive MRI for structural lesions typical of axSpA, the gold standard being majority central reader decision as to the presence of a definite structural lesion typical of axSpA with high confidence.
Methods: MRI structural lesions meeting ASAS definitions from 148 cases were recorded in an eCRF that comprises global assessment (Is there a structural lesion typical of axSpA (yes/no) and degree of confidence (-4 (lesion absent) to +4 (lesion present)), and detailed scoring of lesions per SIJ quadrant and per slice. We calculated sensitivity and specificity for numbers of SIJ quadrants and consecutive slices with erosion, sclerosis, and fat lesions where a majority of readers (≥4/7) agreed as to the presence of a structural lesion typical of axSpA with high confidence (≥ +3). We selected cut-offs with ≥95% specificity. These cut-offs were analyzed for their predictive utility for rheumatologist diagnosis of axSpA at follow up (average of 4.4 years) by calculating positive and negative predictive values (PPV, NPV) and selecting those cut-offs with PPV of ≥95% and comparable predictive utility with global MRI assessment. Both specificity of ≥95% for a definite lesion as well as a PPV of ≥95% were considered requirements for preliminary designation of MRI lesion cut-offs defining a positive MRI for structural lesions.
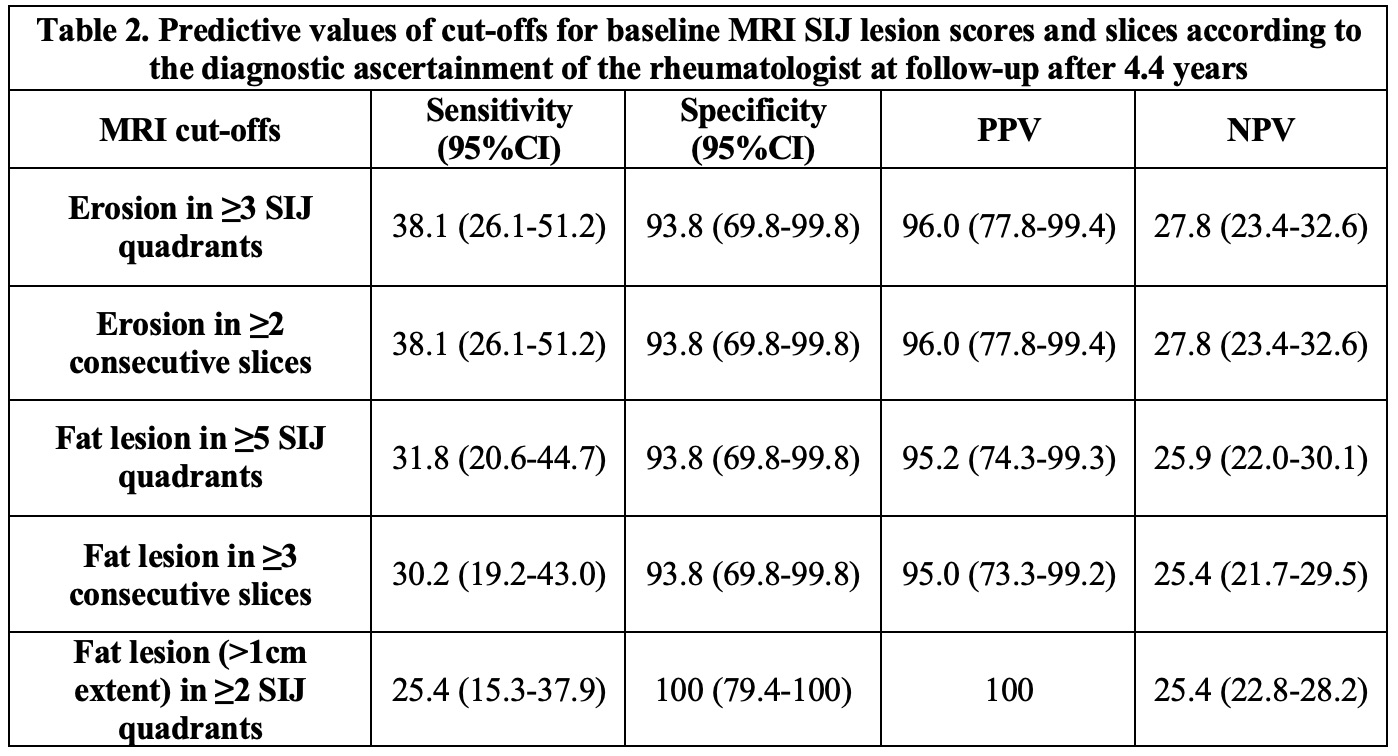
Results: Structural lesions typical of axSpA were observed by majority read in 33 (32.4%) of 102 cases diagnosed with axSpA, and 3 (6.8%) of 44 cases without axSpA and 29 cases were assigned a high degree of confidence (≥ +3) by a majority of readers. Cut-offs achieving specificity of ≥95% for a definite structural lesion were erosion at the same location in ≥2 consecutive slices (sensitivity 83%), erosion at any location in ≥3 SIJ quadrants (sensitivity 90%), fat lesion at any location in ≥5 SIJ quadrants (sensitivity 62%), fat lesion at the same location in ≥3 consecutive slices (sensitivity 52%), and ‘deep’ fat lesion (≥1cm extent) in ≥2 SIJ quadrant (sensitivity 55.2%) (Table 1). All of these had very high positive predictive values (≥95%) for diagnosis of axSpA in cases diagnosed by the rheumatologist after 4.4 years follow up (Table 2). Combinations of cut-offs for different structural lesions were not superior to single lesion cut-offs.
Conclusion: ASAS-defined erosion in ≥2 consecutive slices or in ≥3 SIJ quadrants, and ASAS-defined fat lesion in ≥3 consecutive slices or in ≥5 SIJ quadrants or ‘deep’ fat lesion (≥1cm extent) in ≥2 SIJ quadrants are high priority candidates for defining an MRI structural lesion typical of axSpA. This will require similar assessment in additional axSpA cohorts.
- Maksymowych et al. Ann Rheum Dis 2019; 78:1550-8.
- Rudwaleit et al. Ann Rheum Dis 2009;68: 777-83
- Maksymowych et al. Ann Rheum Dis May 05 2020

To cite this abstract in AMA style:
Maksymowych W, Baraliakos X, Weber U, Machado P, Pedersen S, Sieper J, Wichuk S, Poddubnyy D, Rudwaleit M, van der Heijde D, Landewé R, Paschke J, Lambert R, Østergaard M. Preliminary Definition of a Positive MRI for Structural Lesions in the Sacroiliac Joints in Axial Spondyloarthritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/preliminary-definition-of-a-positive-mri-for-structural-lesions-in-the-sacroiliac-joints-in-axial-spondyloarthritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/preliminary-definition-of-a-positive-mri-for-structural-lesions-in-the-sacroiliac-joints-in-axial-spondyloarthritis/