Session Information
Date: Monday, October 27, 2025
Title: (1306–1346) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) is a frequent extra-articular manifestation of RA predisposing to poor health outcomes. The disease course in RA-ILD is variable, with some patients having stable courses while others experience a more progressive disease course. This variation complicates management decisions, particularly since few predictors of RA-ILD progression have been consistently identified. For example, in some, but not all, prior studies, usual interstitial pneumonia (UIP) ILD pattern has been associated with a more severe disease course. In this study, we aimed to evaluate predictors of RA-ILD progression among participants with ILD in a multicenter, prospective RA cohort.
Methods: We studied RA-ILD patients within the Veterans Affairs Rheumatoid Arthritis registry, a multicenter, prospective cohort of U.S. veterans with RA. RA-ILD was systematically identified, and all cases validated via standardized medical record review, requiring a clinical diagnosis and supportive imaging or biopsy findings. The index date was the later of registry enrollment or ILD diagnosis, to avoid immortal time bias. ILD progression was defined by change in forced vital capacity (FVC; >5% decline over < 3 years follow-up, >10% decline over >3 years of follow-up) or death up to10 years of follow-up. FVC values were obtained from the electronic health record (EHR) manually or with a validated natural language processing (NLP) tool. Candidate predictors included demographics, RA disease characteristics (e.g., autoantibodies, disease activity), and ILD characteristics (e.g., ILD pattern, baseline FVC % predicted). Predictors were obtained from registry and/or EHR data, with ILD pattern determined per treating pulmonologists and/or radiologists. Multivariable Cox regression models were used to identify determinants of progression.
Results: We studied 347 RA-ILD participants (92% male, mean age 69 years, mean ILD duration 1.7 years) (Table 1). Over 1,487 patient-years of follow-up, 205 (59%) RA-ILD patients experienced progression. In unadjusted comparisons, those who experienced ILD progression were more likely male, reported White race, initiated follow-up in earlier calendar years, and were more frequently current smokers, RF positive, used prednisone, and had an UIP ILD pattern (Table 1). Upon multivariable modeling, factors independently associated with RA-ILD progression included older age (per year aHR 1.03 [1.01, 1.05], smoking status (former vs. never aHR 1.60 [1.00, 2.56]; current vs. never aHR 1.98 [1.15, 3.40], calendar year period (2016-2024 vs. 2003-2015 aHR 0.55 [0.38, 0.79), and UIP ILD pattern (vs. non-UIP aHR 1.46 [1.06, 2.02]) (Table 2; Figure 1).
Conclusion: Older age, cigarette smoking history, and UIP ILD pattern were independently associated with RA-ILD progression in this multicenter RA-ILD cohort. These findings may aid in identifying patient subsets most likely to experience ILD progression and who may warrant closer disease monitoring and more aggressive RA-ILD targeted treatment strategies. Additionally, these findings reinforce the importance of smoking cessation in RA-ILD patients.
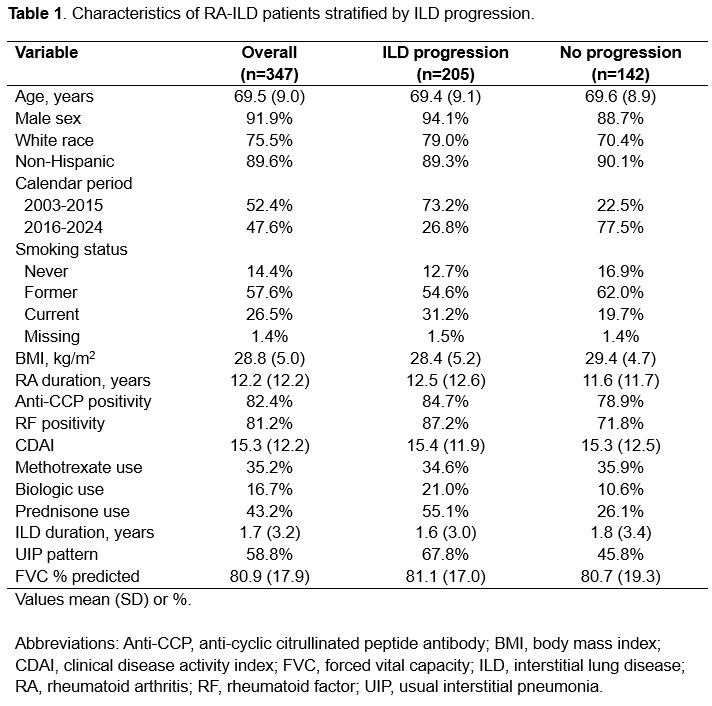 Table 1. Characteristics of RA-ILD patients stratified by ILD progression
Table 1. Characteristics of RA-ILD patients stratified by ILD progression
.jpg) Table 2. Patient characteristics associated with progression in RA-ILD in a multivariable Cox regression model.
Table 2. Patient characteristics associated with progression in RA-ILD in a multivariable Cox regression model.
.jpg) Figure 1. Kaplan-Meier plot of progression-free survival by ILD pattern.
Figure 1. Kaplan-Meier plot of progression-free survival by ILD pattern.
To cite this abstract in AMA style:
England B, Wheeler A, Frideres H, Matson S, Thiele G, Wysham K, Cannon G, Kunkel G, Kerr G, Reimold A, Richards J, Ascherman D, Monach P, Baker J, Mikuls T. Predictors of Interstitial Lung Disease Progression in Patients with Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/predictors-of-interstitial-lung-disease-progression-in-patients-with-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/predictors-of-interstitial-lung-disease-progression-in-patients-with-rheumatoid-arthritis/