Session Information
Date: Saturday, November 6, 2021
Title: Systemic Sclerosis & Related Disorders – Clinical Poster I (0387–0413)
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Connective tissue disease associated interstitial lung disease (CTD-ILD) is associated with decreased quality of life and high mortality risk. Outcome and treatment response is unpredictable. This study aimed to identify clinical predictors for CTD-ILD with poor outcome.
Methods: We performed a retrospective single center cohort study in outpatients with CTD-ILD seen between 2004 and 2018. Clinical, biochemical data as well as pulmonary function test (PFT) and high-resolution computed tomography (HRCT) results were recorded. The ILD patterns were classified according to the classification for idiopathic interstitial pneumonia and categorised into fibrotic or inflammatory. Overall survival and progressive fibrosing ILD (PF-ILD, defined as ≥ 10% decline in FVC, ≥ 15% decline in DLCO, or progression of the fibrosis on HRCT within two years) were assessed.
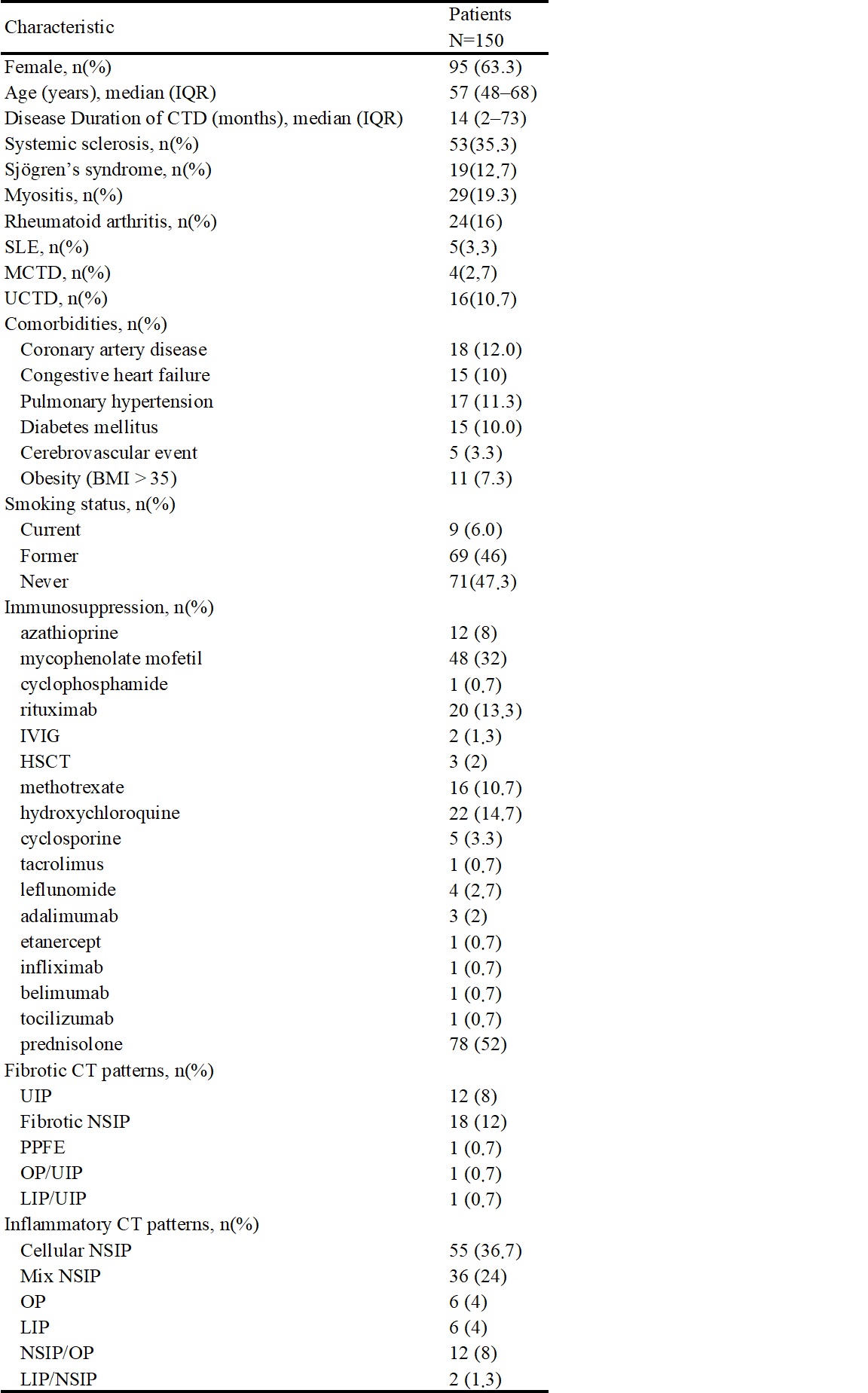
Results: In total, 150 patients with CTD-ILD were included. Table 1 shows the baseline patient characteristics. Thirty (20%) deaths occurred during a median follow-up of 40 months (IQR 27.3–60.8), which were attributed to pulmonary infection in six (4%), respiratory failure due to PF-ILD in ten (7%) and due to other causes in fourteen patients. PF-ILD occurred in 74 (49.3%) patients and was associated with poor overall survival. (Figure 1) Age, smoking, C-reactive protein, and steroid-use were independently associated with increased mortality risk as well. (Table 2) Furthermore, patients with diabetes mellitus (adjusted OR 4.2, 95%CI 1.05–16.78), steroid-use (adjusted OR 2.38, 95%CI 1.09–5.18), and a fibrotic HRCT pattern at baseline (adjusted OR 3.02, 95%CI 1.11–8.24) had a higher risk of PF-ILD.
Conclusion: PF-ILD is associated with increased mortality in patients with CTD-ILD. Patients with a fibrotic HRCT pattern at baseline, diabetes mellitus and steroid-use have a higher risk of developing PF-ILD.


To cite this abstract in AMA style:
Chiu Y, Spierings J, de Jong P, Mohamed Hoesein F, Grutters J, van Laar J, Voortman M. Predictors for Progressive Fibrosis in Patients with Connective Tissue Disease Associated Interstitial Lung Diseases [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/predictors-for-progressive-fibrosis-in-patients-with-connective-tissue-disease-associated-interstitial-lung-diseases/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/predictors-for-progressive-fibrosis-in-patients-with-connective-tissue-disease-associated-interstitial-lung-diseases/