Session Information
Date: Sunday, November 5, 2017
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Despite the pro-thrombotic nature of antiphospholipid antibodies (aPL), thrombocytopenia is frequently observed in patients with antiphospholipid syndrome (APS) or in non-APS patients with aPL. The management of the thrombocytopenia with aPL (aPL related thrombocytopenia; APAT) is often deductive, due to the paradoxical risks of thrombosis and hemorrhage. We have been striving to clarify the mechanisms of APAT and reported its high prevalence of arterial thrombotic events (Nakagawa I, et al. ACR 2014, Abstract #2). In the present study, along with the reconfirmation of the clinical importance of APAT, we aimed to evaluate the efficacy of therapeutic regimes in APAT through a systematic review of the literature with the objective of elaborating a clinical practice guideline for APAT on a consignment project from the Japanese Ministry of Health, Labor and Welfare.
Methods: Four clinical questions were selected for systematic review and redefined using the PICO (Patient, Intervention, Comparison, Outcome) format and prioritized. The four clinical questions were to evaluate the effects of possible therapeutics for APAT; antiplatelet agents, glucocorticoids, splenectomy and thrombopoietin receptor agonists. Systematic reviews were performed using electronic databases (MEDLINE, EMBASE and CENTRAL) by the Cochrane Japan Centre. Cochrane Collaboration Review Manager software was used to manage and analyze the data collected.
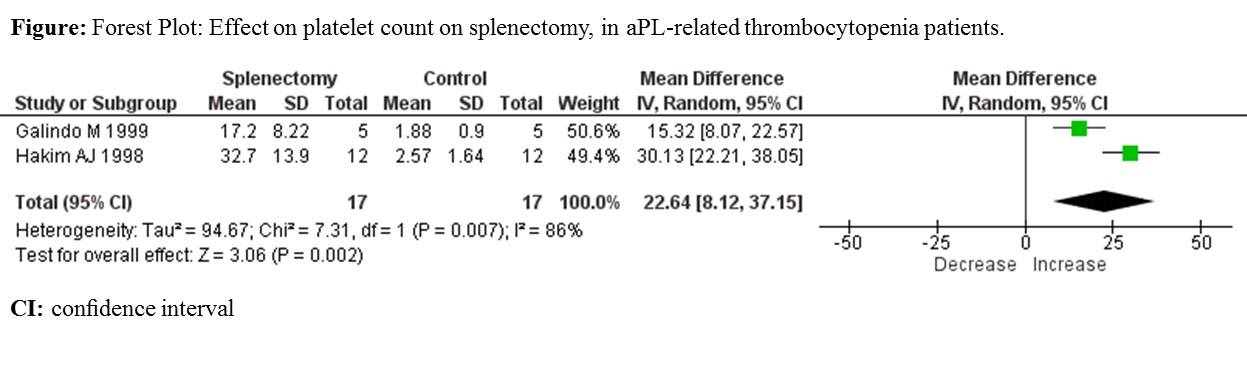
Results: The initial search yielded 1407 citations of which nine were included in our final analysis. There was no randomized controlled trial on treatment for APAT. We identified four case-controlled studies for splenectomy, one for antiplatelet agents and four observational studies for glucocorticoids. Meta-analysis of quantitative data (17/23) showed evidence of an increase in platelet count in patients who underwent splenectomy compared with the patients without splenectomy (mean difference 22.6~104 /mL, P = 0.007) (Figure). Complete remissions of the thrombocytopenia were observed in 18/23 (78%) patients with splenectomy versus 0/23 (0%) without splenectomy. The relapses were occurred in 3/23 (13%) patients with splenectomy. There was no complications due to splenectomy. None of the configured outcomes were susceptible to the antiplatelet and glucocorticoid therapy.
Conclusion: Although splenectomy for APS was previously reported to be a risk of portal vein thrombosis, our systematic review and meta-analysis revealed that it may be performed rather safely and effectively in APAT patients. However, there was no clear evidence to support applications of antiplatelet agents, glucocorticoids, or thrombopoietin receptor agonists as therapeutics of APAT. Further clinical trials are required to establish therapeutic recommendation for APAT.
To cite this abstract in AMA style:
Abe N, Oku K, Amengual O, Fujieda Y, Kato M, Bohgaki T, Yasuda S, Mori R, Morishita E, Suzuki-Inoue K, Atsumi T. Possible Therapeutics for Antiphospholipid Antibody Related Thrombocytopenia: A Systemic Review and Meta-Analysis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/possible-therapeutics-for-antiphospholipid-antibody-related-thrombocytopenia-a-systemic-review-and-meta-analysis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/possible-therapeutics-for-antiphospholipid-antibody-related-thrombocytopenia-a-systemic-review-and-meta-analysis/