Session Information
Date: Sunday, November 13, 2016
Title: Vasculitis - Poster I: Large Vessel Vasculitis and Polymyalgia Rheumatica
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with Giant Cell Arteritis (GCA) have an increased risk of devastating cranial ischaemic complications including vision loss and stroke. The BSR guidelines recommend platelet inhibition with aspirin to reduce the risk of ischaemic complications in GCA. Thrombosis occurs following platelet activation. The glycoprotein VI (GPVI) receptor is found exclusively on platelets and megakaryocytes. The proteolytic cleavage of GPVI occurs following platelet activation and is detectable in the plasma as soluble GPVI (sGPVI). Therefore elevated plasma sGPVI is a marker of platelet activation and a risk marker for adverse cardiovascular outcomes. Enhanced platelet activation is observed in inflammatory arthritis. We hypothesized that GCA would also be associated with platelet hyperreactivity which might support the rationale for aspirin use in GCA.
Methods: Following ethics approval and informed consent, blood samples were taken from patients with GCA. Healthy control samples were obtained from volunteers. Demographic and clinical data were collected for all participants. Blood samples were processed as double spun platelet poor plasma. sGPVI levels were measured using ELISA. sGPVI levels were compared between patients with GCA and healthy controls, between active and inactive GCA, and between those with and without cranial ischaemic compications. Mann-Whitney U test was used to compare groups. Spearman¡¯s Rank Correlation Coefficient was used to assess for associations between sGPVI levels and demographic and clinical markers. GraphPad Prism and SPSS were used for data analysis.
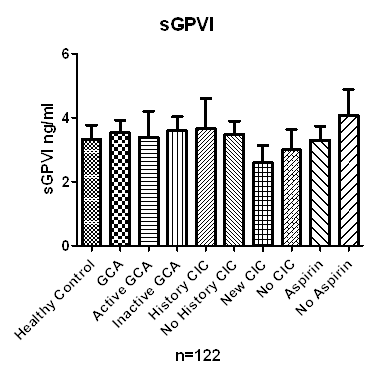
Results: 122 patients were included in the study, 70 with GCA and 53 healthy controls. Of the GCA patients, 19 had active disease and 19 had had cranial-ischaemic complications. There was no difference in sGPVI levels between GCA and healthy controls , median (IQR) 2.32 ng/ml (1.60, 4.21) vs 2.19 ng/ml (1.72, 3.31) (p=0.76). sGPVI levels were similar in GCA patients with active and inactive disease, median 2.31 ng/ml (1.86, 4.21) vs 2.33 ng/ml (1.57, 4.21) (p=0.93). sGPVI levels were similar in GCA patients with and without a history of cranial ischaemic complications, median 2.04 ng/ml (1.33, 4.21) vs 2.37 ng/ml (1.88, 4.21) (p=0.85). sGPVI levels taken from patients at initial presentation with and without cranial ischaemic complications were no different, median 2.31 ng/ml (1.33, 4.21) vs 2.27 ng/ml (1.72, 3.22) (p=0.91). Aspirin therapy did not significantly affect sGPVI levels, median 2.22 ng/ml (1.40, 4.20) vs 2.74 ng/ml (2.01, 4.64). There was no correlation between sGPVI levels and CRP (r=0.16), ESR (r=0.10), or prednisolone dose (r=-0.21).
Conclusion: We found no evidence of increased platelet activation in patients with GCA. There was no association between platelet activation and disease activity or cranial ischaemic complications in GCA. Figure 1: sGPVI levels in GCA
To cite this abstract in AMA style:
Conway R, Madigan A, Helbert L, Redmond N, Dunne E, Molloy ES, Kenny D, McCarthy GM. Platelet Activation, As Measured By Plasma Soluble Glycoprotein VI, Is Not Associated with Disease Activity or Ischaemic Events in Giant Cell Arteritis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/platelet-activation-as-measured-by-plasma-soluble-glycoprotein-vi-is-not-associated-with-disease-activity-or-ischaemic-events-in-giant-cell-arteritis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/platelet-activation-as-measured-by-plasma-soluble-glycoprotein-vi-is-not-associated-with-disease-activity-or-ischaemic-events-in-giant-cell-arteritis/