Session Information
Date: Wednesday, November 8, 2017
Title: Osteoarthritis – Clinical Aspects II: Structural Progression and Incidence
Session Type: ACR Concurrent Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: Epidemiology for hand osteoarthritis (OA) incidence is lacking and few large cohorts have sufficient size to explore subsets. We previously characterized a subset of adults who develop an accelerated form of knee OA, in which they progress from normal radiographic appearance to advance-stage disease within 4 years and often in < 12 months. It is unknown whether such a novel subset exists among adults with hand OA. We aimed to characterize individuals who develop accelerated hand OA (AHOA) and compare them to those who do not.
Methods: We evaluated 3489 participants in the Osteoarthritis Initiative (OAI) with complete data for baseline and 48-month radiographic hand OA. One reader scored posteroanterior radiographs of the dominant hand using a modified Kellgren-Lawrence (KL) scale (weighted kappa > 0.84) and another reader scored the presence of central or marginal erosions (kappa > 0.79). We defined hand OA as a hand with at least 1 joint with KL grade ≥ 2 on at least 2 fingers (digits 2 to 5). We defined AHOA as a hand with at least 1 joint that progressed from a KL grade of 0 or 1 at baseline to KL 3 or 4 at 48 months. We ran descriptive statistics to characterize AHOA.
Results: The overall rate of AHOA was 1.12% over 4 years, with 38 hands having 1 joint affected and 1 hand with 2 joints affected. At baseline, adults who developed AHOA were more likely to have radiographic hand OA (69% vs 36%), central erosions (21% vs 7%), and marginal erosions (8% vs 2%) in other joints compared to those who did not develop AHOA (see Table). Only 1 joint that developed accelerated OA had an erosion (marginal) at baseline. Adults with AHOA were more likely to develop new erosions in either the same or any other joint over 48 months (central n = 13, 34%; marginal n = 3, 8%) than those who did not develop AHOA (central n = 162, 5%; marginal n = 51, 1%). Eight (21%) people who developed AHOA had an incident erosion in the same joint that worsened. Only 1 person (3%) with AHOA had a fracture during the observation period, compared to 48 people (2%) with fractures in the control group. The most common locations of accelerated OA were the thumb and second digit (Figure 1).
Conclusion: Adults who developed AHOA were more likely to have erosive hand OA than those without AHOA, confirming that erosive hand OA is a more rapid progressing phenotype. Furthermore, the majority of those who developed AHOA were affected at the second metacarpophalangeal joint (28%) or the first carpometacarpal joint (26%). This suggests the digits commonly used for pinching and fine motor skills are particularly susceptible to accelerated OA compared to other digits.
|
Table 1. Baseline Characteristics of Adults Who Develop Accelerated Hand Osteoarthritis (OA) |
||
|
|
No Accelerated OA |
Accelerated OA |
|
n = 3489 mean (SD) or n (%) |
n = 39 mean (SD) or n (%) |
|
|
Female n (%) |
2020 (58%) |
24 (62%) |
|
Pre-menopause n (%) |
295 (15%) |
3 (13%) |
|
Peri-menopause n (%) |
291 (14%) |
2 (8%) |
|
Post-menopause n (%) |
1423 (71%) |
19 (79%) |
|
Physician Diagnosed Hand OA n (%) |
581 (17%) |
6 (15%) |
|
Prevalent Hand Pain n (%) |
835 (24%) |
6 (15%) |
|
Radiographic Hand OA n (%) |
1246 (36%) |
27 (69%) |
|
Central Erosions (≥ 1 joint) n (%) |
239 (7%) |
8 (21%) |
|
Marginal Erosions (≥ 1 joint) n (%) |
84 (2%) |
4 (11%)* |
|
Metabolic Syndrome (2-4 components) n (%) |
1933 (58%) |
26 (67%) |
|
Self-Reported Diabetes n (%) |
268 (8%) |
1 (3%) |
|
Use of Lipid Medications n (%) |
988 (28%) |
7 (18%) |
|
High Blood Pressure n (%) |
2110 (60%) |
28 (72%) |
|
Large Waist Circumference n (%) |
2553 (74%) |
31 (79%) |
|
Age (years) |
60.9 (9.2) |
60.6 (9.1) |
|
Body Mass Index (kg/m2) |
28.7 (4.8) |
29.1 (5.0) |
|
Body Weight (kg) |
81.6 (16.4) |
81.2 (15.7) |
|
Notes on missing data: Only included people with body weight, and status of self-reported hand pain (yes or no) and physician diagnosed hand OA (yes and no or unknown) at baseline. Missing data: Less than 3% missing data for menopause status, central erosions, marginal erosions, diabetes status, and waist circumference. Metabolic syndrome (n missing = 137 controls). No other missing data. * 1 marginal erosion occurred in the same joint that developed accelerated hand osteoarthritis and 3 had marginal erosions in a different joint. |
||
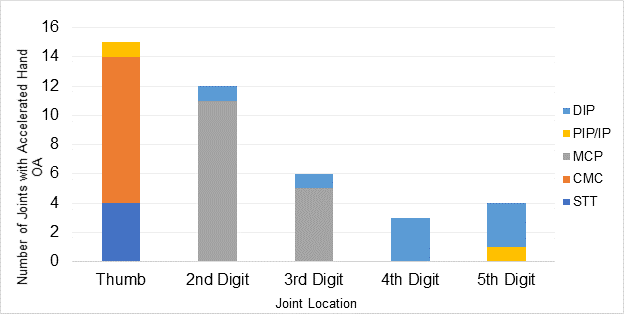
Figure 1. Patterns of Accelerated Hand Osteoarthritis by Location
To cite this abstract in AMA style:
Davis J, Schaefer LF, McAlindon TE, Eaton CB, Roberts M, Haugen IK, Smith S, Duryea J, Lu B, Driban JB. Patterns and Characteristics of Accelerated Hand Osteoarthritis: Data from the Osteoarthritis Initiative [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/patterns-and-characteristics-of-accelerated-hand-osteoarthritis-data-from-the-osteoarthritis-initiative/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patterns-and-characteristics-of-accelerated-hand-osteoarthritis-data-from-the-osteoarthritis-initiative/