Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Interstitial lung disease (ILD) is a significant cause of morbidity and mortality in idiopathic inflammatory myopathies (IIM) as well as systemic sclerosis (SSc). The purpose of this study is to compare the prevalence, physiology, and radiographic findings in IIM as well as to analyze the utilization of screening/monitoring plans in different clinical and antibody defined patient subsets.
Methods: Patients diagnosed with polymyositis (PM), dermatomyositis (DM), anti-aminoacyl tRNA synthetase syndrome (ARS), limited cutaneous systemic sclerosis (lcSS), or diffuse cutaneous systemic sclerosis (dcSS) were identified from the MYSTIC cohort (VUMC IRB 141415) and using subject locator (VUMC IRB 180672). The presence of ILD was identified from chart abstraction. Radiographic patterns of ILD were ascertained from the initial CT scan. American Thoracic Society (ATS) criteria were used to grade severity of lung disease by forced vital capacity (FVC) and diffusion lung capacity for carbon monoxide (DLCO) percentages. If multiple pulmonary function tests (PFTs) were available, the most severe value was used. Symptom onset was defined as the start of any clinical manifestation of IIM or SSc.
Results: Patient characteristics are shown in Table 1. Sixty-nine of 131 patients had ILD with the highest prevalence in ARS (81.5%) and dcSS (71.4%). Overall, most patients had CT morphology other than usual interstitial pneumonia (UIP) (Table 2). Non-Jo1 (45.5%) ARS were most frequently classified as UIP. Severe restriction was present in 36.4% of Jo-1+ and 63.6% of non-Jo-1 ARS patients, compared with 33.3% of dcSS patients. Similarly, 72.7% of ARS patients (54.5% Jo-1+ and 90.9% non-Jo-1) and 55.6% of dcSS had severe gas exchange deficits. Supplemental oxygen use was 25.9% in ARS and 14.3% in dcSS. Despite the prevalence of ILD at 45% and 43.9% in lcSS and DM, respectively, physiologic severity was less than for ARS or dcSS. FVC was severely restricted in only 12.5% of lcSS cases and 5.6% of DM cases. Over 62% of lcSS patients had severe reduction in DLCO, but this is likely due to concomitant pulmonary hypertension. The time from symptom onset to first PFT or HRCT was the shortest with the ARS group (Figure 1). ARS patients (72.7%), particularly the non-Jo-1 ARS (100%), were more likely than other groups (34%) to be seen first in pulmonary clinic.
Conclusion: In our cohort, ARS had the highest prevalence and severity of ILD. ARS patients, especially non-Jo-1 ARS patients, were more likely to be seen initially in pulmonary clinic and receive earlier screening for ILD. However, these patients may also have delayed diagnosis due to lack of extra-pulmonary symptoms thus presenting with more severe disease. Implementing routine screening for ARS in pulmonary clinics may identify patients earlier and change management.

Table 1
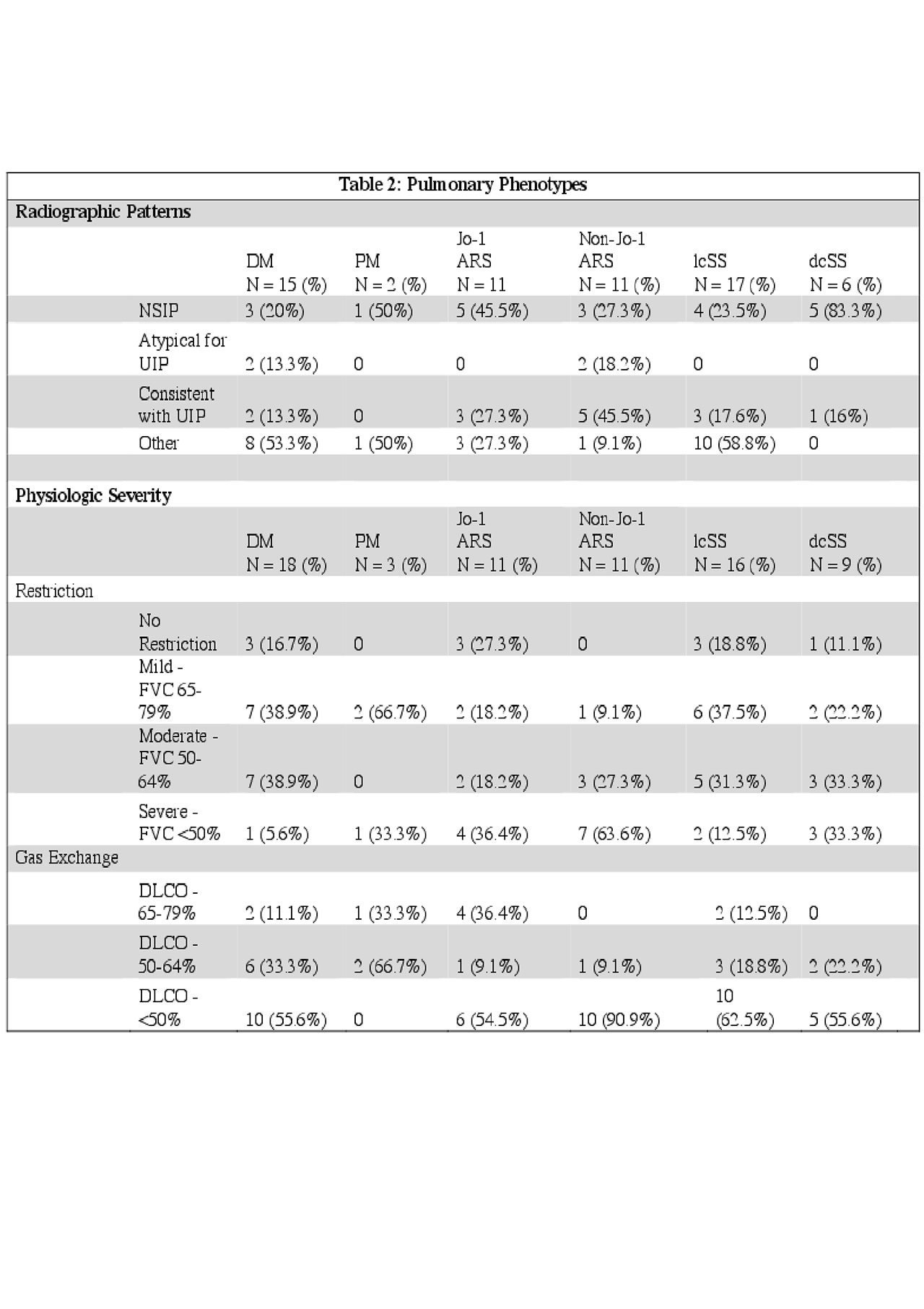
Table 2
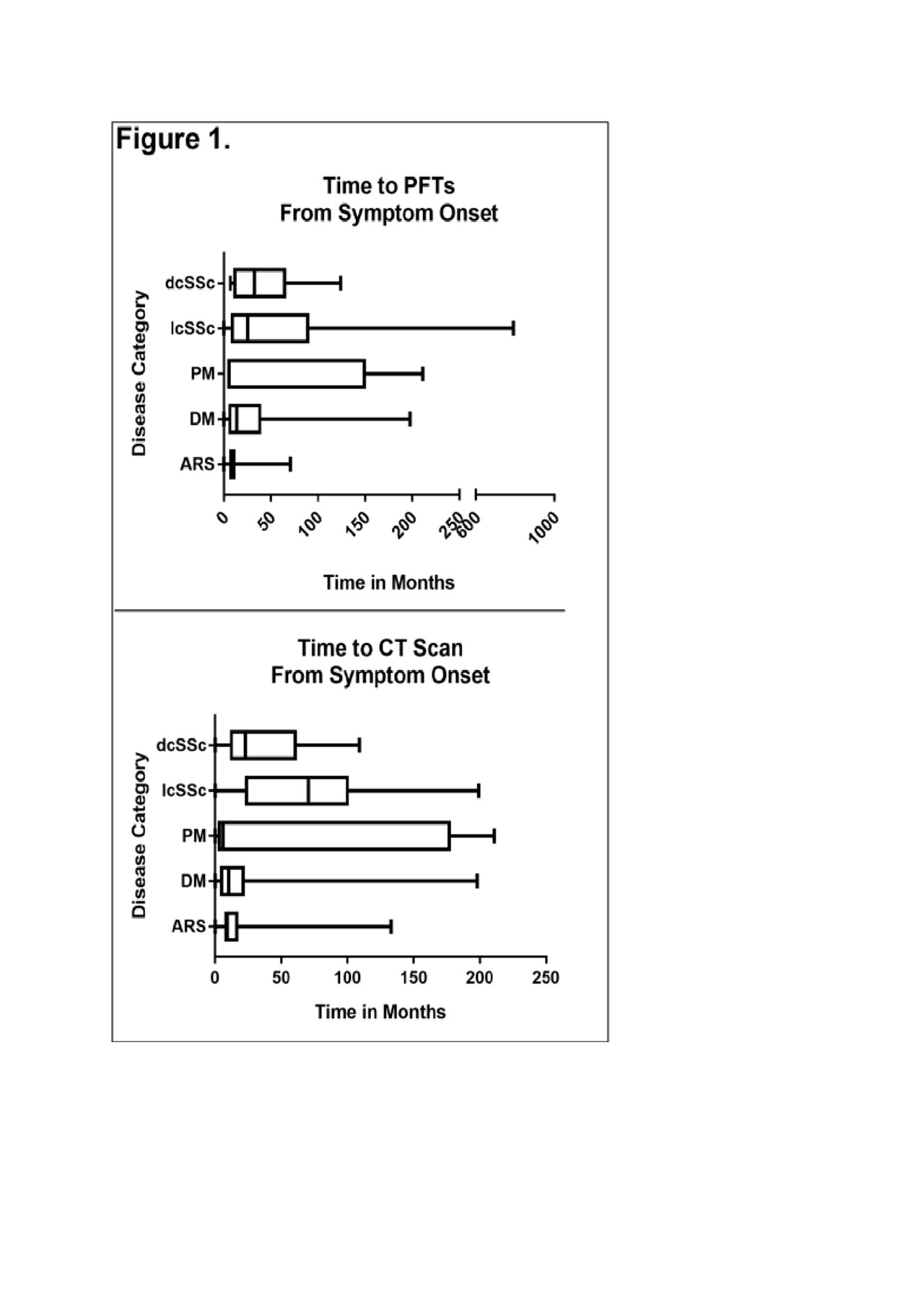
Figure 1
To cite this abstract in AMA style:
Sohn B, Wilfong E, Crofford L. Patients with Anti-tRNA Synthetase Syndrome Are More Likely to Present to Pulmonary Clinic and Have a Higher Prevalence and Severity of Lung Disease Than Patients with Other Types of Myositis or Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/patients-with-anti-trna-synthetase-syndrome-are-more-likely-to-present-to-pulmonary-clinic-and-have-a-higher-prevalence-and-severity-of-lung-disease-than-patients-with-other-types-of-myositis-or-syste/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patients-with-anti-trna-synthetase-syndrome-are-more-likely-to-present-to-pulmonary-clinic-and-have-a-higher-prevalence-and-severity-of-lung-disease-than-patients-with-other-types-of-myositis-or-syste/