Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Familial Mediterranean Fever (FMF) is a genetic disorder characterized by recurrent febrile episodes and inflammation, most commonly presenting with peritonitis, pleuritis, and arthritis. The study investigates the varied pathways to FMF, exploring the duration from symptom onset and diagnostic processes among a cohort of participants.
Methods: This study involved surveying patients at an autoinflammatory clinic to explore the diagnostic pathways leading to the identification of FMF.
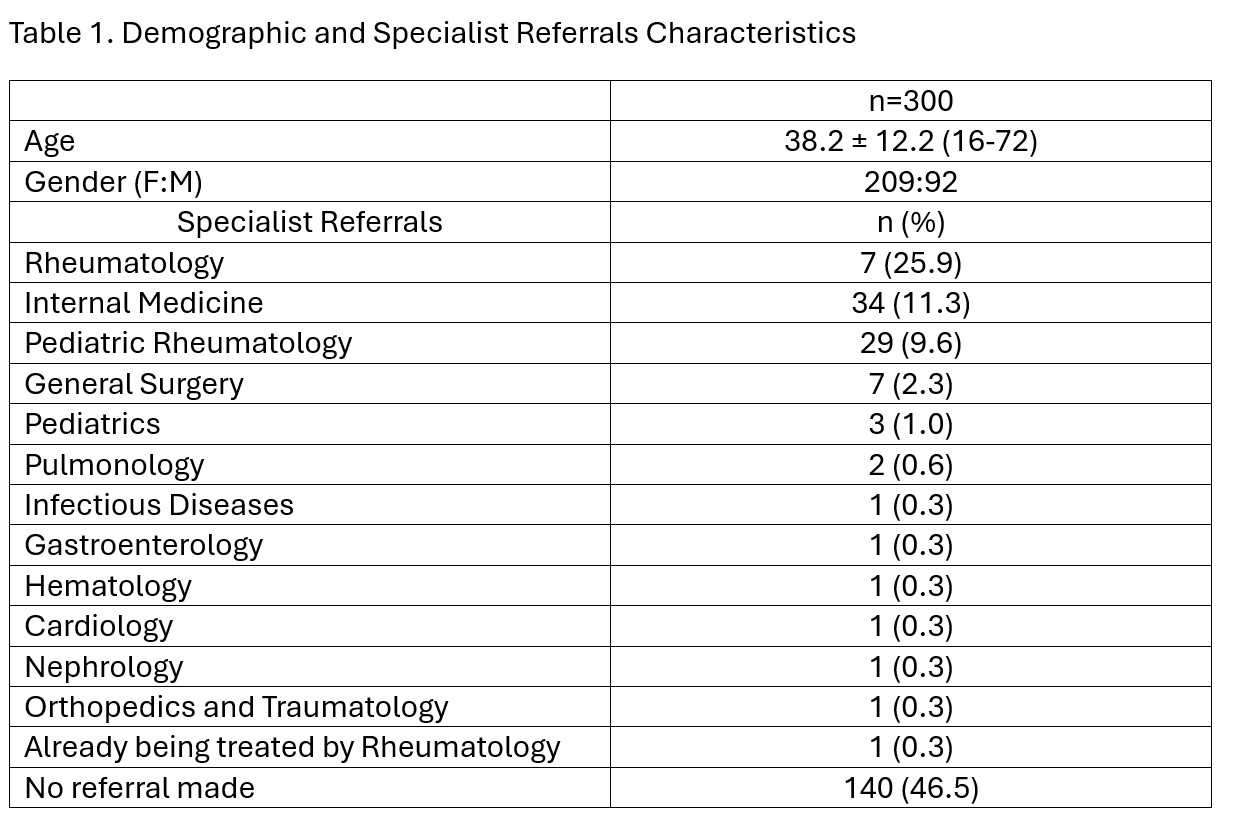
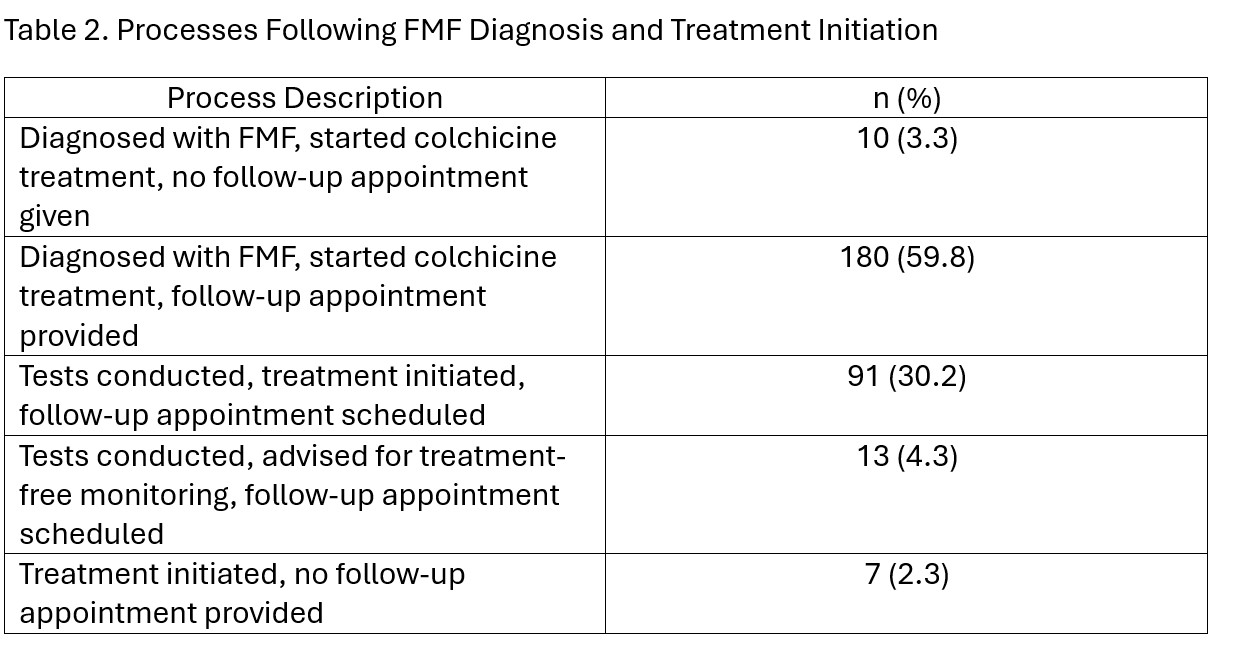
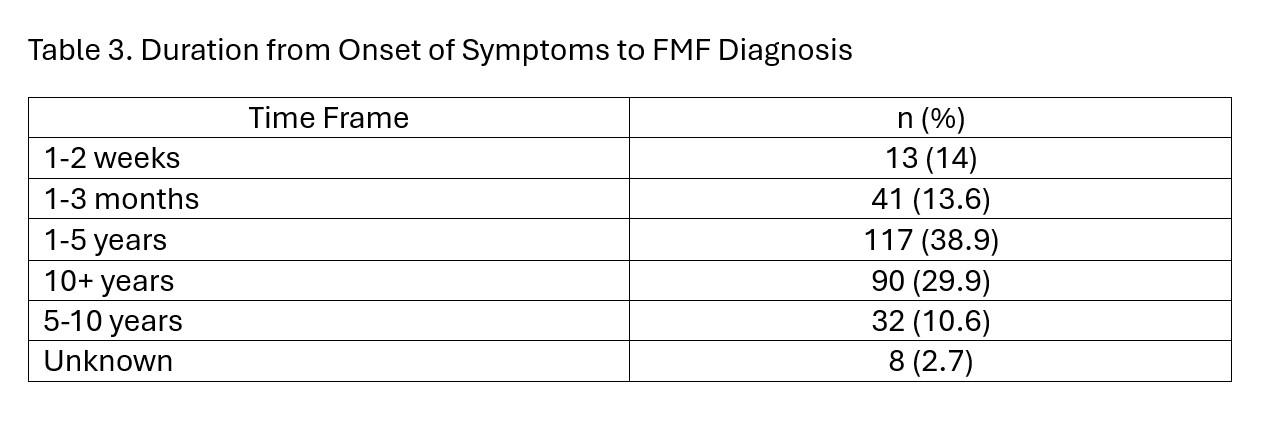
Results: A sample of 300 patients with a mean age of 38.2 years (± 12.2 years, range 16-72), consisting of 209 males and 92 females was examined. (Table 1.) Before their FMF diagnosis, patients consulted various specialties: 38.9% with internal medicine, 18.9% with pediatrics, and 15.3% with emergency medicine. Additionally, 26.7% consulted other departments. Regarding referrals, 47.5% were referred to another specialty, while 52.5% were not. Among the participants, 25.9% were initially referred to rheumatology. 46.5% did not receive any initial referral. (Table 1.) In the initial consultation with the rheumatologist, 59.8% received an FMF diagnosis and started colchicine treatment with a follow-up appointment scheduled. (Table 2.) 38.9% waited between 1 to 5 years from the onset of initial symptoms to their diagnosis by the rheumatologist for FMF. (Table 3.) Following the diagnosis of FMF, 31.9% of patients continued their follow-up with the doctor who initially diagnosed them, while 68.1% did not continue with the diagnosis doctor. After receiving a diagnosis of FMF, treatment for FMF typically started within one day for 68.6% of patients, 14.0% began treatment within 1-2 weeks, 6.6% within 1 month, 3.7% within 1-3 months, and 7.0% started treatment after 3 months or more. After starting their first FMF preventive medication, 68.4% experienced four or more attacks requiring additional medication. Additionally, 8.3% had two episodes, 4.7% had three episodes, and another 4.7% had one episode. 14.0% did not experience any attacks after starting treatment. 89.7% secured appointments with their rheumatologist in less than a week, while 7.0% experienced waits exceeding a month. 17.9% of participants reported trying alternative approaches, while 82.1% did not pursue alternative treatments. 49.5% expressed confidence regarding future improvement in their condition, 31.9% were not optimistic, and 18.6% were uncertain.
Conclusion: These findings highlight varied initial consultations for FMF, showing significant diagnosis delays and frequent changes in healthcare providers post-diagnosis, emphasizing the need for standardized protocols to improve care continuity.
To cite this abstract in AMA style:
Karup S, Polat D, Dincsoy E, Azman F, Cokrak M, Berkiten E, Ugurlu S. Path to Diagnosis in Familial Mediterranean Fever (FMF) [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/path-to-diagnosis-in-familial-mediterranean-fever-fmf/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/path-to-diagnosis-in-familial-mediterranean-fever-fmf/