Session Information
Date: Sunday, November 17, 2024
Title: Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Controversy exists surrounding the association of gout with osteoporosis diagnosis or incident fragility fractures. Dual-Energy X-Ray Absorptiometry (DXA) scan is the gold standard for diagnosing osteoporosis and osteopenia. This study aimed to compare the prevalence of osteoporosis and osteopenia by DXA in patients with and without gout in in a large academic health care system.
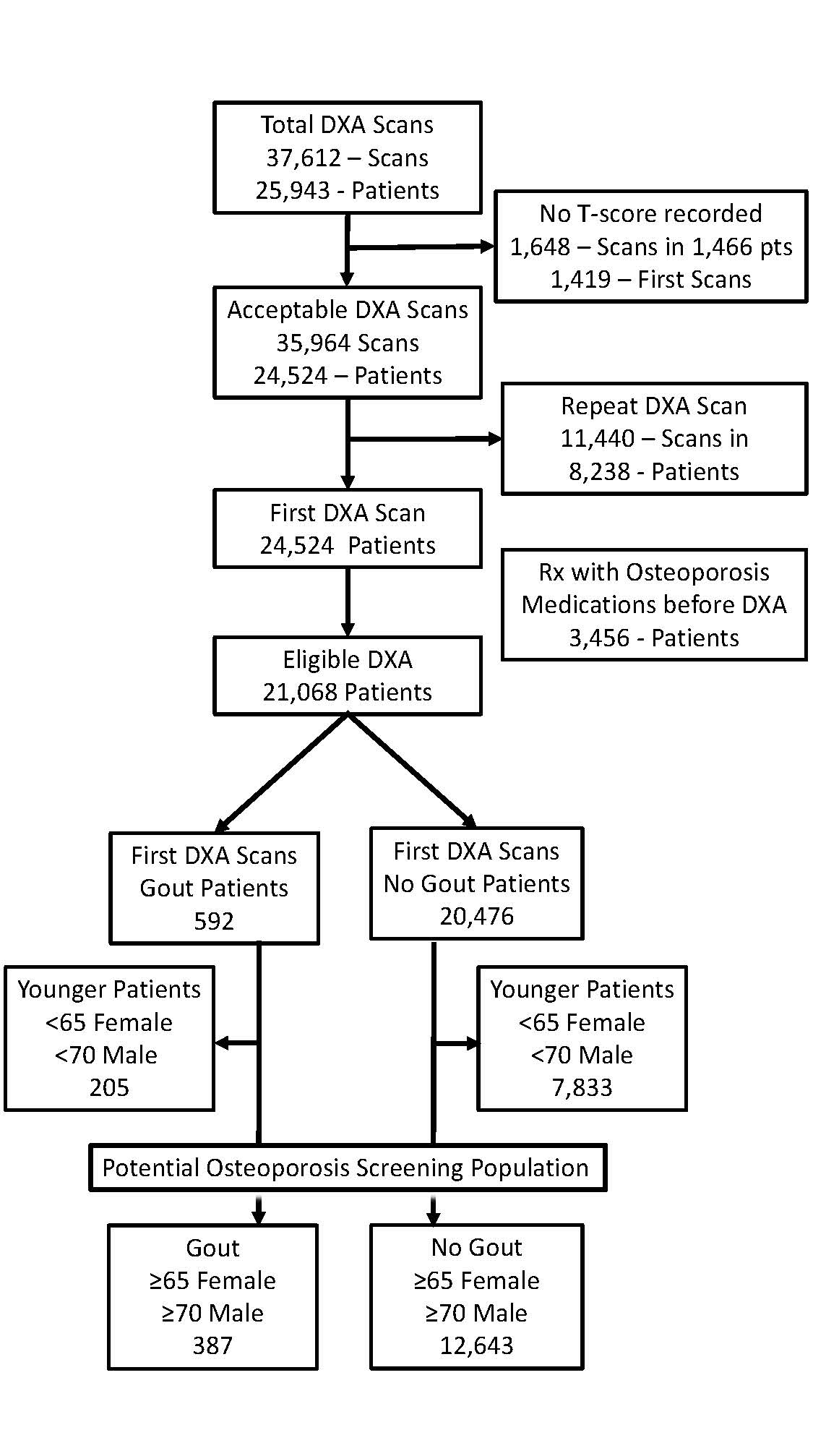
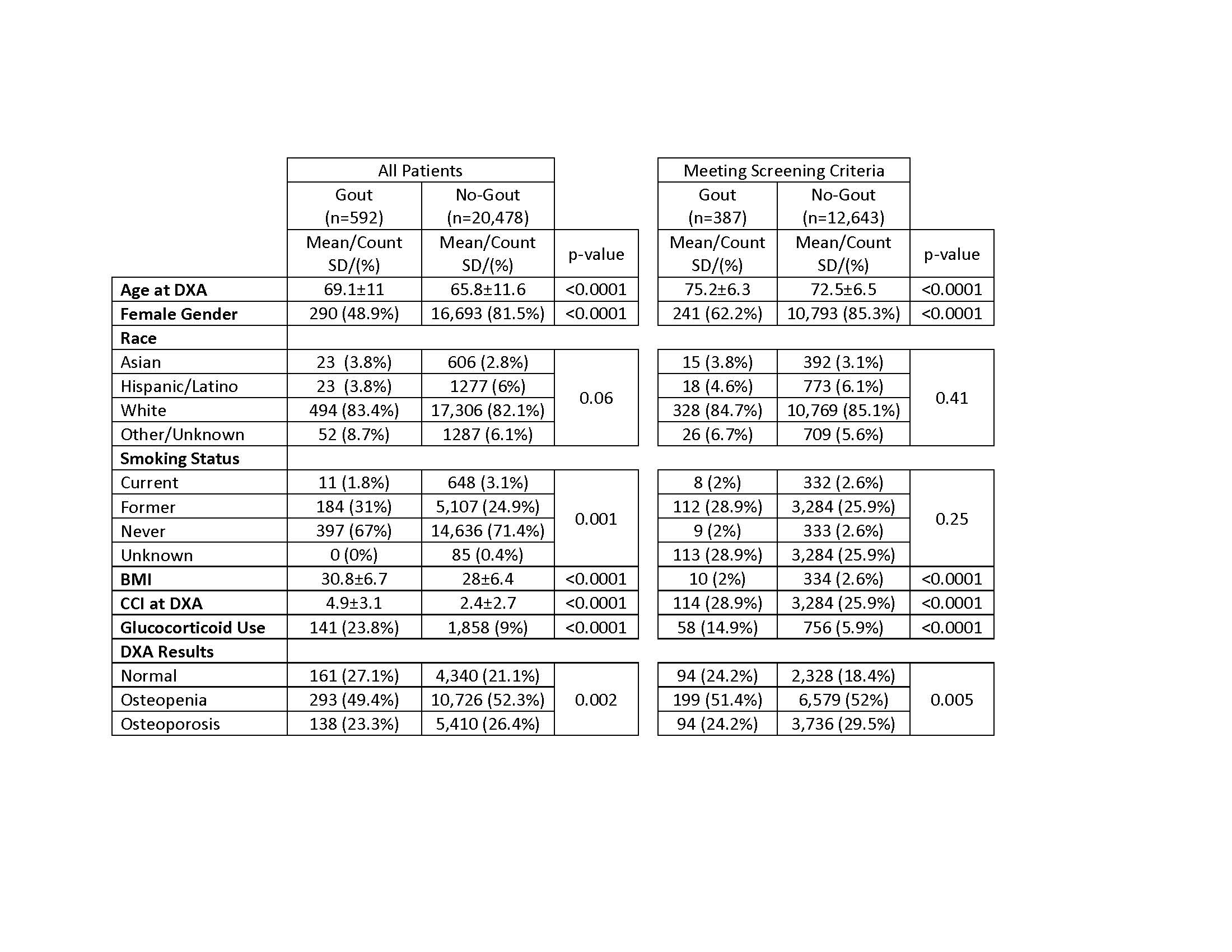
Methods: All patients having DXA scans between January 1, 2015, and June 30, 2023, were identified as “Gout” or “No Gout” based on the presence or absence of one or more Gout ICD-10 codes before DXA (Figure 1). For each patient, DXA T-score results at either the total hip, femoral neck, spine, and/or radius on the first DXA were classified as normal bone density, osteopenia, or osteoporosis based on World Health Organization criteria. Demographic and clinical features evaluated were age at DXA, body mass index (BMI), Charlson co-morbidity index (CCI) at DXA, glucocorticoid use, self-reported gender, race, and smoking. Glucocorticoid exposure was defined as ≥90 days of glucocorticoid with an average daily dose of ≥5 mg prednisone equivalent per day prior to and/or active prescription at the time of DXA to simulate the glucocorticoid risk used in FRAX. A subpopulation analysis for patients “Meeting Screening Criteria” evaluated patients who met the age-based DXA screening criteria for females and males. “Gout” patients were compared to “No Gout” patients using logistical regression with crude and adjusted odds ratios reported.
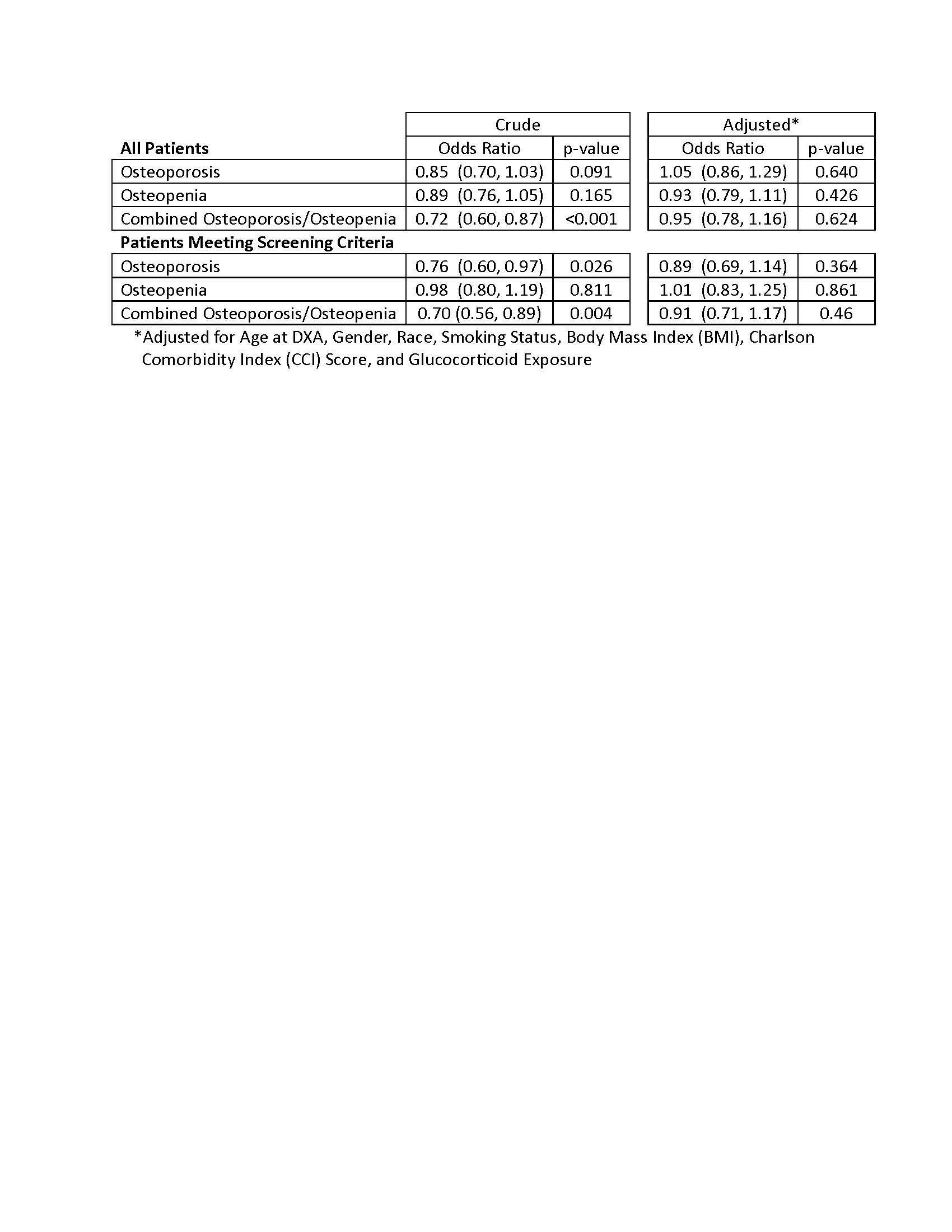
Results: Of the 21,068 eligible first DXA studies performed, there were 592 “Gout” and 20,476 “No Gout” patients, and in the screening population subgroup, there were 387 “Gout” and 12,643 “No Gout” patients (Figure 1). Gout patients were older, more frequently male, predominantly white with small differences in race distribution, had higher BMI, higher CCI, higher glucocorticoid use, and less osteoporosis and osteopenia in both the total population and subpopulation of “Meeting Screening Criteria” (Table 1). Gout in the total population was associated with significantly less combined osteoporosis/osteopenia in the crude analyses (OR 0.72, p-value < 0.001) but was no longer significant when adjusted for age, gender, race, smoking status, BMI, CCI, and glucocorticoid exposure (Table 2). Gout in the “Meeting Screening Criteria” subpopulation was associated with significantly less osteoporosis (OR 0.76, p-value 0.26) and combined osteoporosis/osteopenia (OR 0.70, p-value 0.004) in crude analyses, but differences were no longer significant in the adjusted analyses (Table 2).
Conclusion: This is the first study to use DXA scans to diagnose osteoporosis in gout patients. In this cross-sectional analysis, we found that the diagnosis of osteoporosis and osteopenia, using DXA scans, was not increased in patients with gout in our full population or those “Meeting Screening Criteria.” In gout patients, higher comorbidities such as CCI score and glucocorticoid use could be associated with osteoporosis, but the association might be mitigated in part by higher BMI in this population.
To cite this abstract in AMA style:
Miller K, Cannon g, Register K, Grant N, Schlesinger N. Osteoporosis and Osteopenia Diagnosed by Dual-Energy X-Ray Absorptiometry Are Not Increased in Patients with Gout [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/osteoporosis-and-osteopenia-diagnosed-by-dual-energy-x-ray-absorptiometry-are-not-increased-in-patients-with-gout/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/osteoporosis-and-osteopenia-diagnosed-by-dual-energy-x-ray-absorptiometry-are-not-increased-in-patients-with-gout/