Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Many studies have documented gaps in quality of care for knee and hip osteoarthritis (OA), particularly with respect to lifestyle (e.g., weight management, exercise) and rehabilitative therapies. Key drivers of these patterns include the lack of standardized models for OA management and the limited time available during clinic visits to address non-pharmacological aspects of care. Given these challenges, we conducted an exploratory trial of an OA Clinic-Community CARE Model (OA CARE).
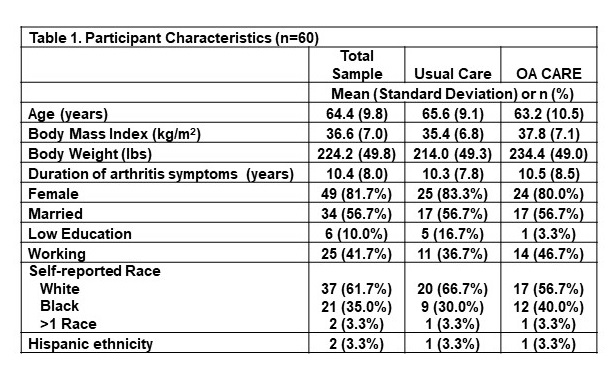
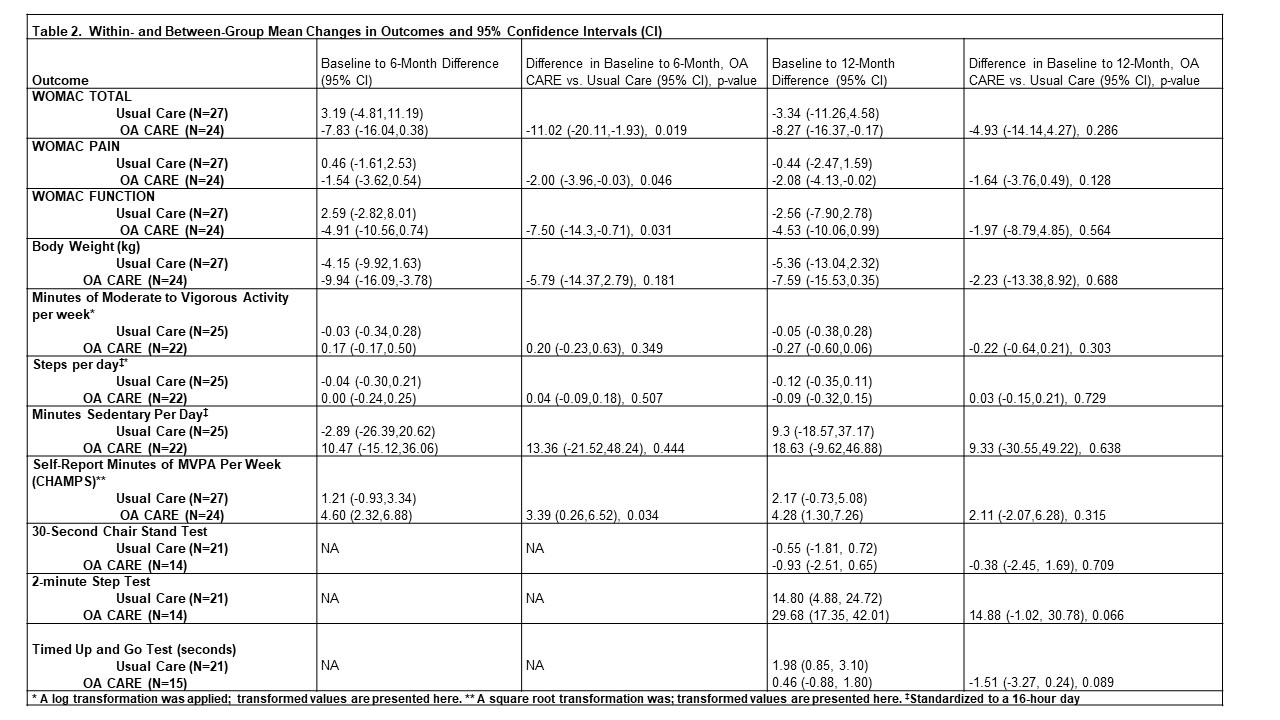
Methods: Participants (n=60) with symptomatic knee or hip OA and body mass index ³ 27 were randomized to OA CARE or a usual care control group (UC). The OA CARE group received a 12-month medical membership to a local YMCA, which included a 12-week weight management program and access to exercise equipment and classes. These participants were also provided with tailored referrals to physical therapy, additional weight management services, sleep-related services and psychological services. Primary care clinicians of these patients were given a video-based summary of OA treatment guidelines and collaborated on patients’ referrals to services described above. Outcomes were assessed at baseline, 6-months and 12-months. The primary outcome was the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total score. Between- and within-group changes in outcomes at follow-up time points were compared using general linear mixed effects models.
Results: Participant characteristics are shown in Table 1. In the OA CARE group 26/30 participated in the YMCA weight loss program, with an average attendance of 9/12 sessions, and 17/30 participated in an exercise class. Eight OA CARE group participants received physical therapy during the study period, with few (≤2) accessing other services described above. Within- and between-group mean changes in outcomes are shown in Table 2. At 6-month follow-up, there was a statistically significant difference in change in WOMAC total score, with the OA CARE group showing greater improvement. At 12-months, the between-group change in WOMAC total score was not statistically significant, though there was a small difference in favor of the OA CARE Group. There were also changes in favor of the OA CARE group for multiple secondary outcomes, but the only statistically significant difference was self-reported physical activity at 6 months.
Conclusion: OA CARE is a light-touch care model that is feasible to implement in primary care settings, partnering with a community program to deliver lifestyle components. Effects of OA CARE were modest, and longer or more intensive weight management and exercise programming may be needed to enhance impacts.
To cite this abstract in AMA style:
Allen K, Arbeeva L, Callahan L, Combs K, Godfrey T, Golightly Y, Hales D, Hill C, Huffman K, Nelson A, Rees J, Schwartz T. Optimizing Osteoarthritis Care Through Clinical and Community Partnership: Results of an Exploratory Trial [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/optimizing-osteoarthritis-care-through-clinical-and-community-partnership-results-of-an-exploratory-trial/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/optimizing-osteoarthritis-care-through-clinical-and-community-partnership-results-of-an-exploratory-trial/