Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients who persistently frequent the ED are more likely to be prescribed opioids for pain, and opioid initiation in the ED has been found to increase the risk of long-term opioid therapy (LOT). Pain is frequently experienced by SLE patients, and a major cause of ED use. We sought to understand the prevalence of, and factors associated with opioid dispensation among SLE patients who persistently frequent the ED to identify opportunities to improve quality of care.
Methods: We identified SLE patients who persistently frequented the ED from 2013-2016 at a large urban academic medical center. Persistent use was defined as having three or more ED visits during the 12 months in a calendar year, for at least two out of the four years, consecutive or non-consecutive, during the study period. We collected patient-level variables including demographics and LOT use. Each encounter was categorized as either SLE-, infection-, pain-related or other. Additional encounter-level variables such as healthcare resource utilization and disposition were recorded. We used mixed effects logistic regression to analyze patient- and encounter-level factors associated with opioid administration in the ED and opioid prescription upon discharge from the ED. Variables with p-value <0.1 in univariate analysis were included in a multivariate model.
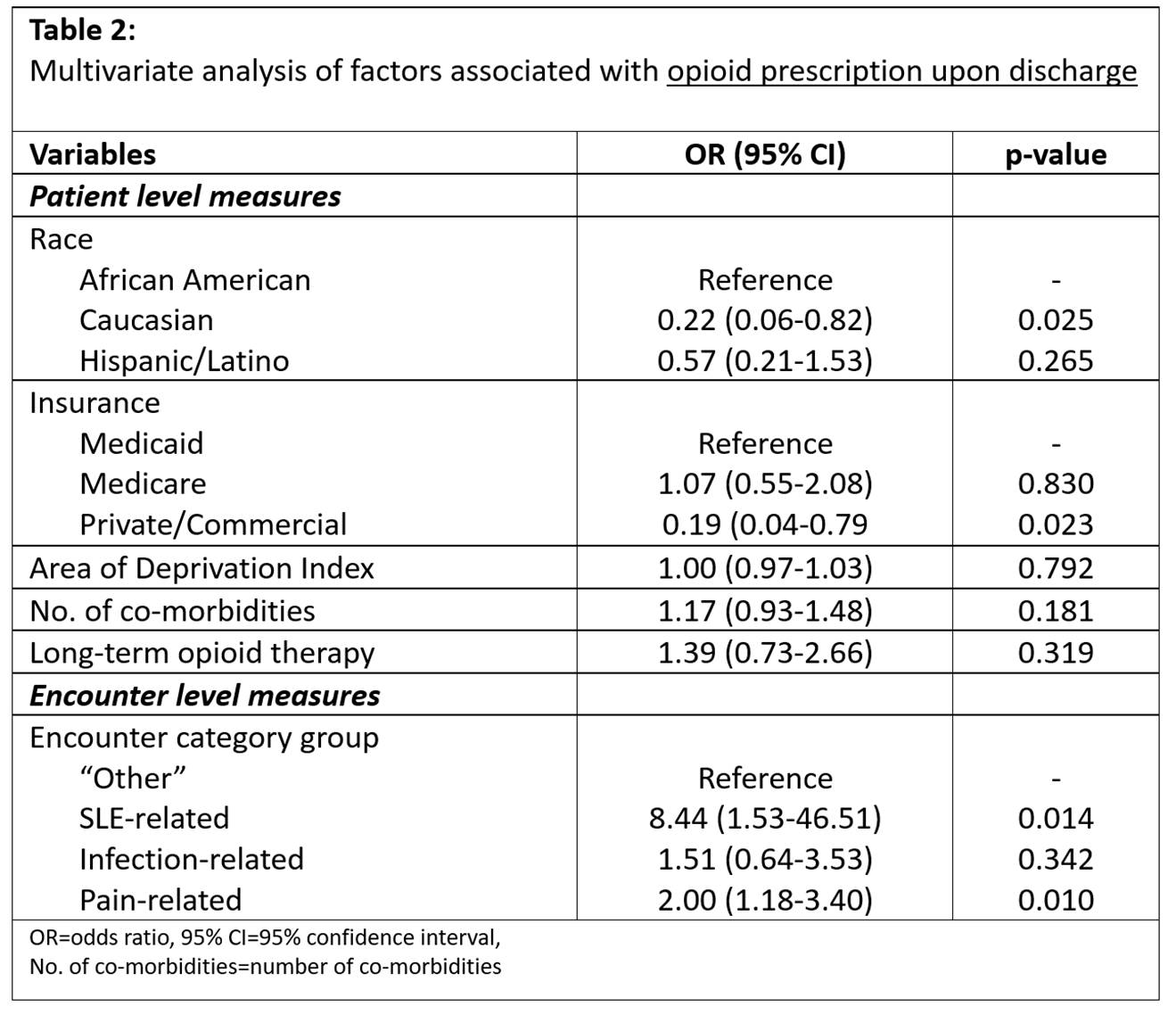
Results: Seventy-seven SLE patients had 1143 ED encounters. Opioids were administered in the ED for 38.4% of all encounters. In multivariate analysis, Medicaid, LOT use, MD as the ED provider (proxy measure for higher acuity), more imaging tests, and rheumatology evaluation were associate with increased odds of opioid administration in the ED (Table 1). Opioids were prescribed on discharge for 16.8% of encounters discharged from the ED. In multivariate analysis, African American patients, those on Medicaid, and patients utilizing the ED for SLE-related activity/complications were more likely to receive an opioid prescription upon discharge from the ED, than their respective counterparts (Table 2).
Conclusion: Opioids are commonly dispensed from the ED for SLE patients, even for those utilizing the ED for lupus-related activity/complications. Further study is warranted to inform how best to decrease opioid use in SLE patients both in the ED and upon discharge.

To cite this abstract in AMA style:
Lee J, Suter LG, Fraenkel L. Opioid Dispensation Among Systemic Lupus Erythematosus (SLE) Patients Who Persistently Frequent the Emergency Department (ED) [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/opioid-dispensation-among-systemic-lupus-erythematosus-sle-patients-who-persistently-frequent-the-emergency-department-ed/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/opioid-dispensation-among-systemic-lupus-erythematosus-sle-patients-who-persistently-frequent-the-emergency-department-ed/