Session Information
Session Type: ACR Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Differentiating smouldering disease activity from weakness due to fatty replacement of atrophied muscle can often be a challenge in Idiopathic Inflammatory Myositis (IIM). There is dearth of biomarkers that can distinguish active from inactive myositis.
To identify changes in metabolomics profiles in serum, urine and muscle of patients with myositis with active and inactive disease. Since we have previously found exquisite separation between paired serum samples obtained in fasting and non-fasting state, only sera collected in fasting state were taken for analysis.
Methods: Sera (n=116), urine (n=114) and muscle (n=11) from patients classifiable as myositis by the ACR-EULAR criteria [34 years (23.5 – 50.5 IQR), M/F 28:88] were compared with healthy controls [n=18 and 12 respectively, age= 44 (35-50) years, M/F-8:10]. For the muscle biopsies, two disease controls were used for comparison. To study effect of fasting state on urine metabolomics, 50 paired urine samples obtained in fasting and non-fasting states were analysed. Metabolic profiles were obtained at 800 MHZ NMR spectrometer and compared using multivariate partial least-squares discriminant analysis (PLS-DA). The discriminatory metabolites were identified based on variable importance in projection (VIP) statistics and further evaluated for statistical significance (p-value < 0.05). Paired T tests were done for metabolites in urine and muscle after normalizing for creatinine. MDAAT >=1 was used to define active myositis.
Results: Metabolomics profiles in IIM were distinct from healthy controls (Fig. 1A). Sera of patients with active myositis exhibited differential clustering from those with inactive myositis (Fig. 1B) with lower amino-acid metabolites (Fig. 1C) elevated phenylalanine-to-tyrosine ratio and glutamate to glutamine ratio (Fig. 1D) and low creatinine (Fig. 1E) with significant discriminatory potential (Fig. 1F). Urine of myositis patients exhibited higher creatine and lower urea and creatine than healthy controls (Fig. 1A, B). However, urine metabolomics exhibited similar clustering in active and inactive disease (Fig. 1C). In urine, paired samples in fasting and non-fasting state exhibited overlapping clustering (Fig. 1D) apart from higher creatine and creatinine (Fig. 1E) . Muscle of patients with inflammatory myositis exhibited almost absent levels of sucrose, mannose, uridine, histamine, inosineand carnitine compared with infection associated myositis.
Conclusion: Serum and urine metabolomics of myositis is distinctive. Serum metabolomic profiling using NMR has the potential to discriminate active from inactive myositis patients though urine metabolomics is largely non-contributory. Muscle metabolites holds potential to distinguish inflammatory myositis from infectious polymyositis.

Figure 1 ACR metabolomics
-A- 3D score plot obtained from PCA analysis of 1D 1H CPMG NMR based serum metabolic profiles showing clustering and separation between Healthy control and inflammatory myositis patients -B- 2 D score plot after PCA analysis of sera from myositis patients with active and inactive disease -C- screening of metabolites responsible for the group separation in the score plot identified based on variable importance in projection -VIP- score > 2.0 -D- VIP projection suggesting elevated phenylalanine-to-tyrosine ratio -PTR- and Glutamate to Glutamine ration -EQR- -E- VIP projection suggesting creatinine is significantly decreased in the sera of active myositis patients -F- representative ROC curves of discriminatory metabolites
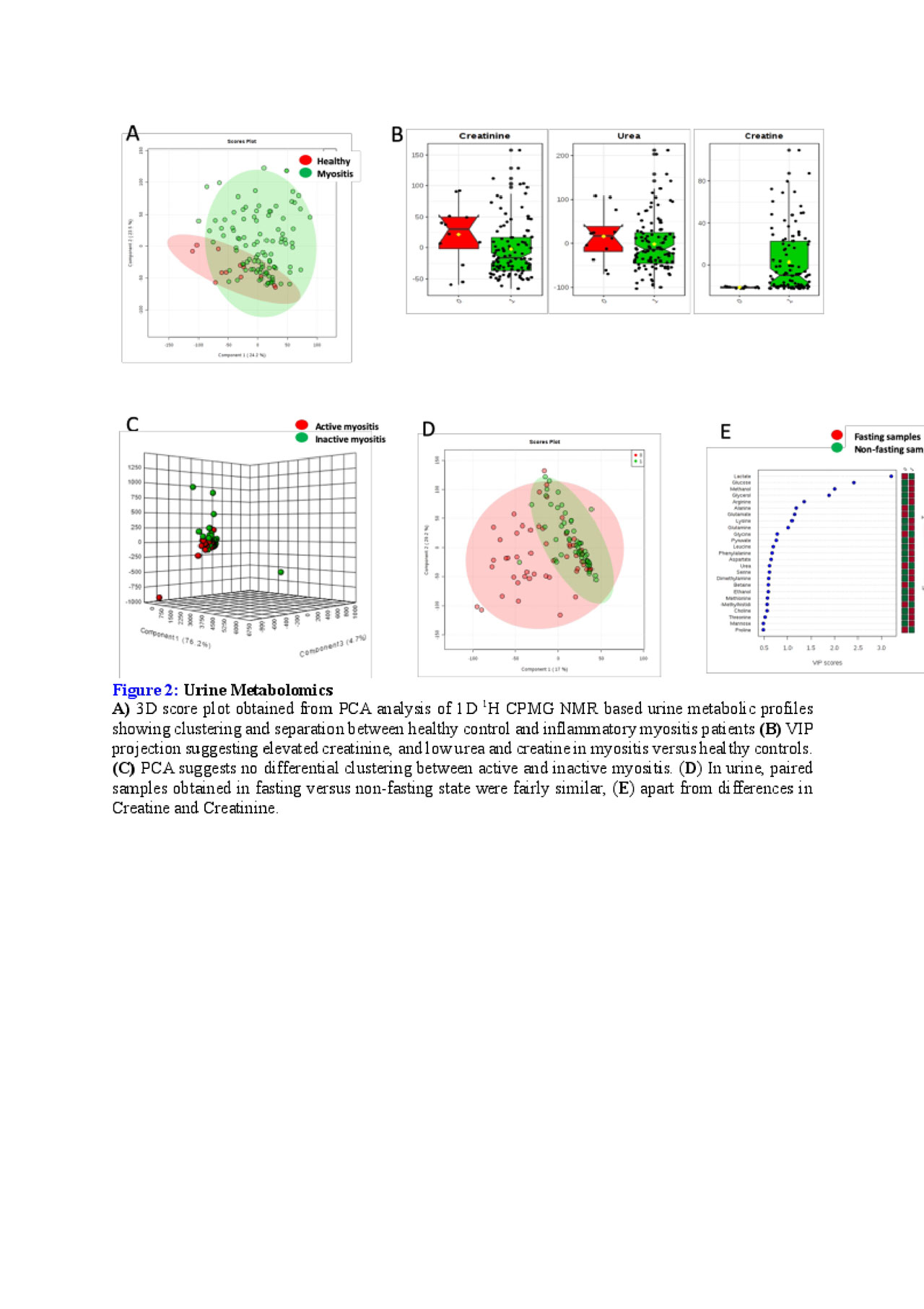
Figure 2 ACR metabolomics
A- 3D score plot obtained from PCA analysis of 1D 1H CPMG NMR based urine metabolic profiles showing clustering and separation between healthy control and inflammatory myositis patients -B- VIP projection suggesting elevated creatinine, and low urea and creatine in myositis versus healthy controls. -C- PCA suggests no differential clustering between active and inactive myositis. -D- In urine, paired samples obtained in fasting versus non-fasting state were fairly similar, -E- apart from differences in Creatine and Creatinine.
To cite this abstract in AMA style:
Gupta L, Kumar D, Kumar U, Guleria A, Zanwar A, Raj R, Misra R. NMR-Based Serum, Urine and Muscle Metabolomics in Inflammatory Myositis for Diagnosis and Activity Assessment: Serum Metabolomics Can Differentiate Active from Inactive Myositis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/nmr-based-serum-urine-and-muscle-metabolomics-in-inflammatory-myositis-for-diagnosis-and-activity-assessment-serum-metabolomics-can-differentiate-active-from-inactive-myositis/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/nmr-based-serum-urine-and-muscle-metabolomics-in-inflammatory-myositis-for-diagnosis-and-activity-assessment-serum-metabolomics-can-differentiate-active-from-inactive-myositis/