Session Information
Date: Monday, November 14, 2016
Title: Rheumatoid Arthritis – Clinical Aspects - Poster II: Co-morbidities and Complications
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose:
Symptomatic heart failure (HF) and HF-associated mortality rates are higher in RA compared with the non-RA population, even after controlling for coronary artery disease (CAD)1, indicating that factors other than flow-limiting CAD contribute to HF in RA. Chronic myocarditis may be one mechanism that contributes to HF in RA. We hypothesized that RA patients without clinical cardiovascular disease (CVD) would have a higher prevalence of subclinical myocarditis compared with non-RA controls, and that it may improve with disease modifying therapy (DMARDs).
Methods : RA patients without prior CV events and with an inadequate response to methotrexate (MTX) underwent a baseline (T1) cardiac [18F-fluorodeoxyglucose (FDG)] positron emission-computed tomography (FDG PET-CT) and a repeat scan six months later following initiation of step-up therapy (T2). Non-RA controls were recruited for a baseline scan only. Myocardial FDG uptake, a measure of myocardial inflammation, was assessed using INVIA Corridor 4DM software and calculated as the global maximum standardized uptake values (SUV max). Participants also underwent 3-D echocardiography to assess left ventricular (LV) mass, volumes, and systolic and diastolic function.
Results : 12 RA patients were enrolled but only 8 completed both scans. 25% received triple therapy and 75% anti-TNF therapy (with background MTX). 12 non-RA controls were enrolled and scanned. Characteristics of RA patients were: 87.5% female, mean age 61± 7.6 years; mean disease duration 5±7 months, 62% seropositive. Controls were younger (mean age 53±12.2) and with fewer women (75%). Mean DAS28-CRP decreased from 4.57±0.31 at T1 to 3.51± 0.41 at T2 (p=0.036. At T1, mean global myocardial SUV max was significantly higher in RA compared with controls (7.2 vs. 3.4 units, respectively; p=0.021). At T2, mean global myocardial SUV max decreased in the RA group, and was now not significantly different from controls at baseline (Figure). Measures of left ventricular (LV) Ejection Fraction (LVEF) and LV mass (LVM) were in normal ranges for both the RA patients and controls with no significant differences between groups. There were no significant changes in LVEF or LVM from T1 to T2 in RA patients.
Conclusion: Patients with active RA exhibited significantly higher myocardial 18FDG-uptake when compared to controls. Improvements in disease activity were paralleled by improvement in myocardial FDG uptake. Larger long-term studies are necessary to determine whether myocardial inflammation is a major risk factor for myocardial dysfunction and HF. Figure: 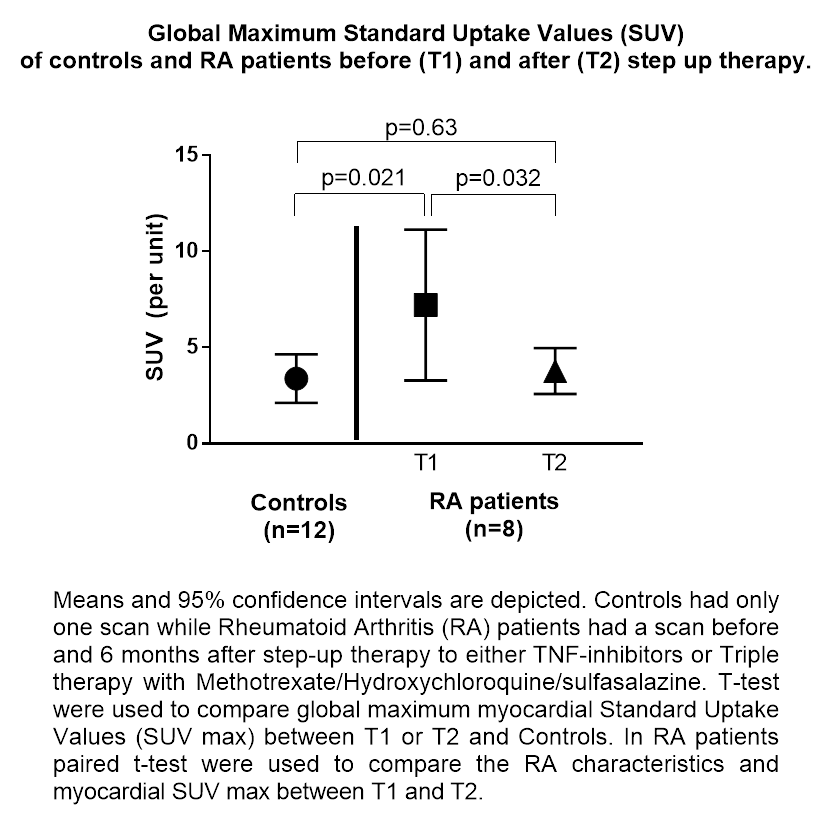
To cite this abstract in AMA style:
Amigues I, Giles JT, Zartoshti A, Morgenstern R, Flores R, Bokhari S, Bathon J. Myocardial 18f-Fluorodeoxyglucose (18F-FDG) Uptake in RA Patients without Clinical Cardiovascular Disease Is Higher Than in Controls and Decreases with Treatment [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/myocardial-18f-fluorodeoxyglucose-18f-fdg-uptake-in-ra-patients-without-clinical-cardiovascular-disease-is-higher-than-in-controls-and-decreases-with-treatment/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/myocardial-18f-fluorodeoxyglucose-18f-fdg-uptake-in-ra-patients-without-clinical-cardiovascular-disease-is-higher-than-in-controls-and-decreases-with-treatment/