Session Information
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: MRI Osteoarthritis Knee Score (MOAKS) is a semi-quantitative scoring system used to assess MRI-detected structural abnormalities including over 100 raw scores representing multiple joint tissues, different ordinal grades and joint subregions or locations. Our objective was to compare 8 different representations of MOAKS in terms of prediction performance for time to incident radiographic OA over 10 years of follow-up.
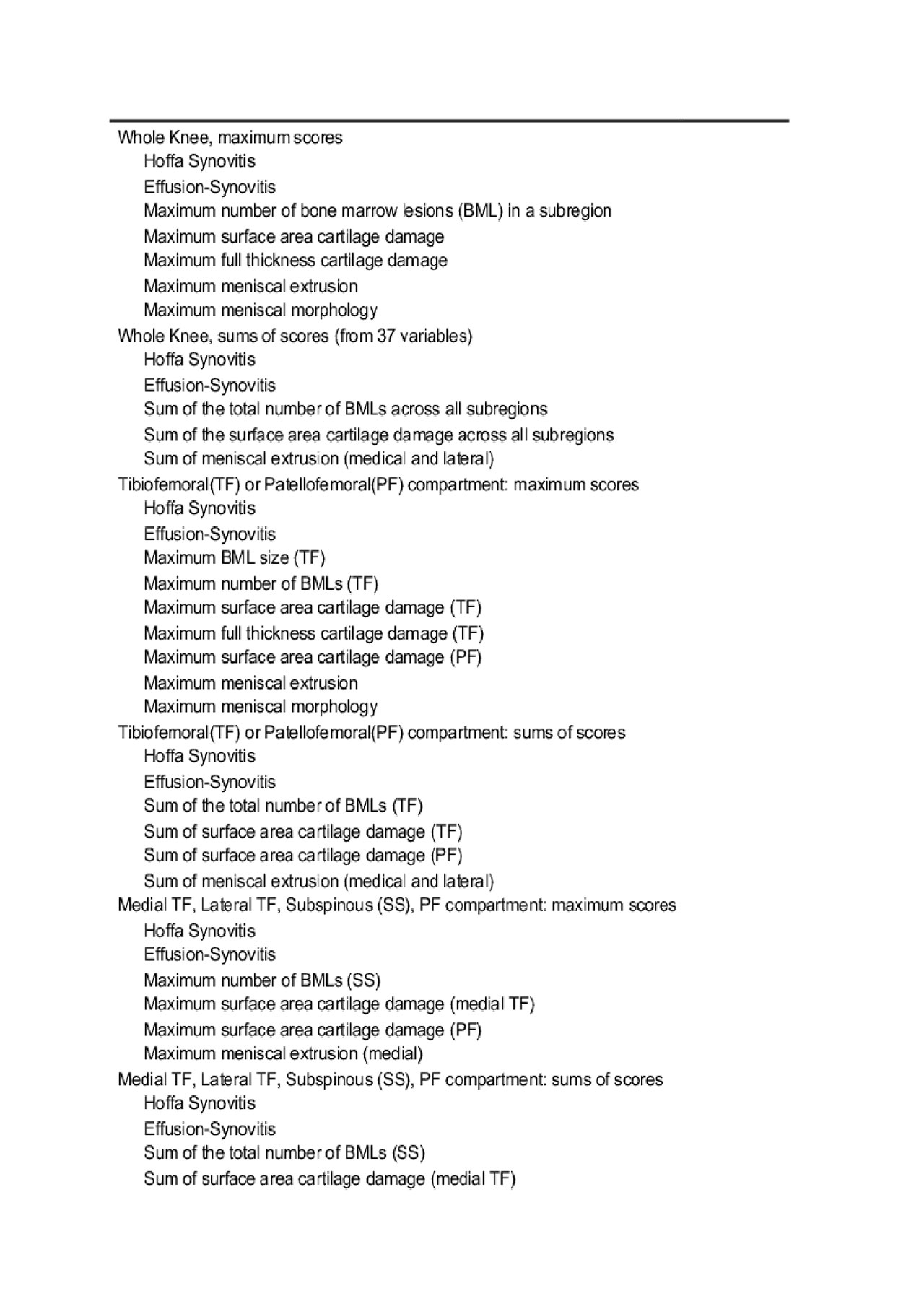
Methods: We randomly selected 859 OAI participants with at least one knee at risk of developing ROA (i.e., KL 0,1 at baseline). 3T knee MRIs were assessed by expert readers using MOAKS. Radiographs were centrally read for KL grade, with ROA defined as KL³2. The 8 representations of MOAKS included features summarized at the whole knee level, the tibiofemoral and patellafemoral (PF) level, and the medial, lateral, subspinous, and PF level, with either maximum scores or sums for ordinal scores of the same feature/type (e.g., maximum number of BML lesions in a subregion (maxBMLLes]); additionally, raw scores as linear predictors and raw scores with indicators for each category were also included.
For each MOAKS representation, we fit lasso penalized Cox models and selected the penalty parameter that achieved a partial log-likelihood deviance within one standard error of the minimum in 10-fold cross validation. Performance of the optimal regularized model was then evaluated with a .632+ bootstrap estimate of the time-dependent Brier score, a weighted mean squared error for predicted survival probability and observed survival status, as well as area under the time-dependent ROC curve.
Results: A total of 244 knees developed incident ROA over the 10 year follow-up. Prediction error based on the area under the estimated prediction error curve was similar for the 8 representations of MOAKS. Variables selected under 6 of 8 representations of MOAKS are shown in Table 1. Performance and model interpretation for the whole knee maximum score model are shown in Figures 1 and 2. Prediction error increased over the course of follow-up (Figure 1a), with the greatest area under the time-dependent ROC curve achieved at 1 and 2 year follow-up (Figure 1b). The nomogram shows the MOAKS variables selected in the model, with the point values for each score, and the correspondence between the total points from these features out of a maximum of 350 points and the 2 year probability of survival from ROA (Figure 2a). For example, a total of 260 points from the 7 variables in the whole knee maximum score model corresponds to a .7 probability of not having ROA 2 years later. Estimated probability of ROA over 10 years is shown for knees with risk scores above and below the median total risk score (Figure 2b).
Conclusion: Different representations of MOAKS, whether maintaining granular-level information or summarizing at the whole knee level with maximum scores or sums of scores, have similar prediction performance for incident ROA. MRI-detected abnormalities provide the greatest discrimination between knees that do and do not develop ROA in the short term (1-2 years), while providing the greatest improvement in prediction over long-term follow-up.
Inc ROA Table 1 rev 3

The blue line is the estimated prediction error curve over 10 years based on the Kaplan-Meier survival estimate, without incorporating any MOAKS data
The black line is the .632+ bootstrap estimate of prediction error based on the Cox model with MOAKS predictors
The red line is the apparent estimate of prediction error -in the full sample- based on the Cox model with MOAKS predictors
1b Area under time-dependent ROC curve for whole knee maximum scores model with bootstrapped 95% confidence bands

2b Predicted Probability of ROA for low risk and high risk knees based on the whole knee maximum scores model; knees with risk scores below the median are “low risk”, while knees with risk scores above the median are “high risk”.
To cite this abstract in AMA style:
Kwoh C, Roemer F, Ashbeck E, Hu C, Bedrick E, Sharma L, Guermazi A. MRI-detected Abnormalities in Prediction Models of Incident Radiographic Knee Osteoarthritis over 10 Years of Follow-up [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/mri-detected-abnormalities-in-prediction-models-of-incident-radiographic-knee-osteoarthritis-over-10-years-of-follow-up/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/mri-detected-abnormalities-in-prediction-models-of-incident-radiographic-knee-osteoarthritis-over-10-years-of-follow-up/