Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), include Granulomatosis with Polyangiitis (GPA), Microscopic Polyangiitis (MPA), and Eosinophilic Granulomatosis with Polyangiitis (EGPA). Mortality rates are scare, Sims et al observed a morality rate of 38.4/1000 person-years (PY) between 2002-2017 (during 3385 PY of follow-up). Moreover, this depends on the AVV subtype, severity of the cohorts studied and their different classification criteria.Our aim is to determine the mortality rate and the main causes of death in patients with GPA, MPA, and EGPA in a region of northern Spain.
Methods: Observational study of AAV from January 1, 2000, to December 31, 2024, in a northern Spanish. Classification of AAV was based on the 2022 ACR/EULAR criteria. Mortality rates were expressed as cases by 106 habitants/year (95% IC) and the Case Fatality rate expressed as percentage (95% IC) of deceased patients. Rates of mortality are expressed as the exposure-adjusted incidence rate (EAIR) per 100 person-years (PY). We defined two patient groups: 1) Study group (deceased patients) and 2) Control group (surviving patients) to compare the main clinical characteristics between these two groups. In addition, we evaluated the principal causes of death among the different types of ANCA-associated vasculitis.
Results: We included 194 patients (99 men/95 women); mean age, 63.7±14.6 years, distributed as follows: GPA (n=67; 34.5%), MPA (n=69; 35.6%), and EGPA (n=28; 14.4%). Death was observed in 56 patients (28.9%); MPA (n=34; 60.7%), GPA (21; 37.5%), and EGPA (1; 3.5%).After a mean of 6±5.4 years of follow up; in AAV group the overall mortality rate was 5.5 per 106 inhabitants/year (95% CI: 3.8-7.1); EAIR of 4.6/100 PY and the overall case-fatality rate was 32.5% (95% CI: 21.9-43.1). Among the AAV subtypes, MPA showed the highest mortality and case-fatality rates with 2.8/106 inhabitants/year (95% CI: 1.7-4); EAIR: 7.9/100 PY and 38.8% (95% CI: 20.1-57.5), respectively. GPA followed with a mortality rate of 1.8/106 inhabitants/year (95% CI: 0.9-42.7); EAIR: 3.86/100 PY and a case-fatality rate of 31.9% (95% CI: 14-49.9). EGPA had low rates: a mortality rate of 0.1/106 habitants/year (95% CI: −0.1-0.2); EAIR: 0.6/100 PY and a case-fatality rate of 1% (95% CI: −1-3) (Table).The main causes of death were infections (n=17; 30%), neoplasia (n=8; 14%), major adverse cardiac events (MACE); (n=7; 13%), renal complications (n=6; 11%), and non-infectious pulmonary complications (n= 4; 7%). Infections were the most frequent cause of death in both GPA and MPA. In EGPA, the only cause of death was MACE. Statistically significant differences were observed between the study group (deceased patients) and the control group (survivors), particularly regarding clinical manifestations associated with a higher risk of mortality, such as pulmonary and renal involvement.
Conclusion: Mortality rates and case-fatality rates in patients with AAV remain relatively high. mortality rate was higher in MPA and lower in EGPA. The most common causes of death were infections (30%), neoplasia (14%), and MACE (13%). Life-threatening organ involvement, such as pulmonary or renal disease, increases mortality risks.
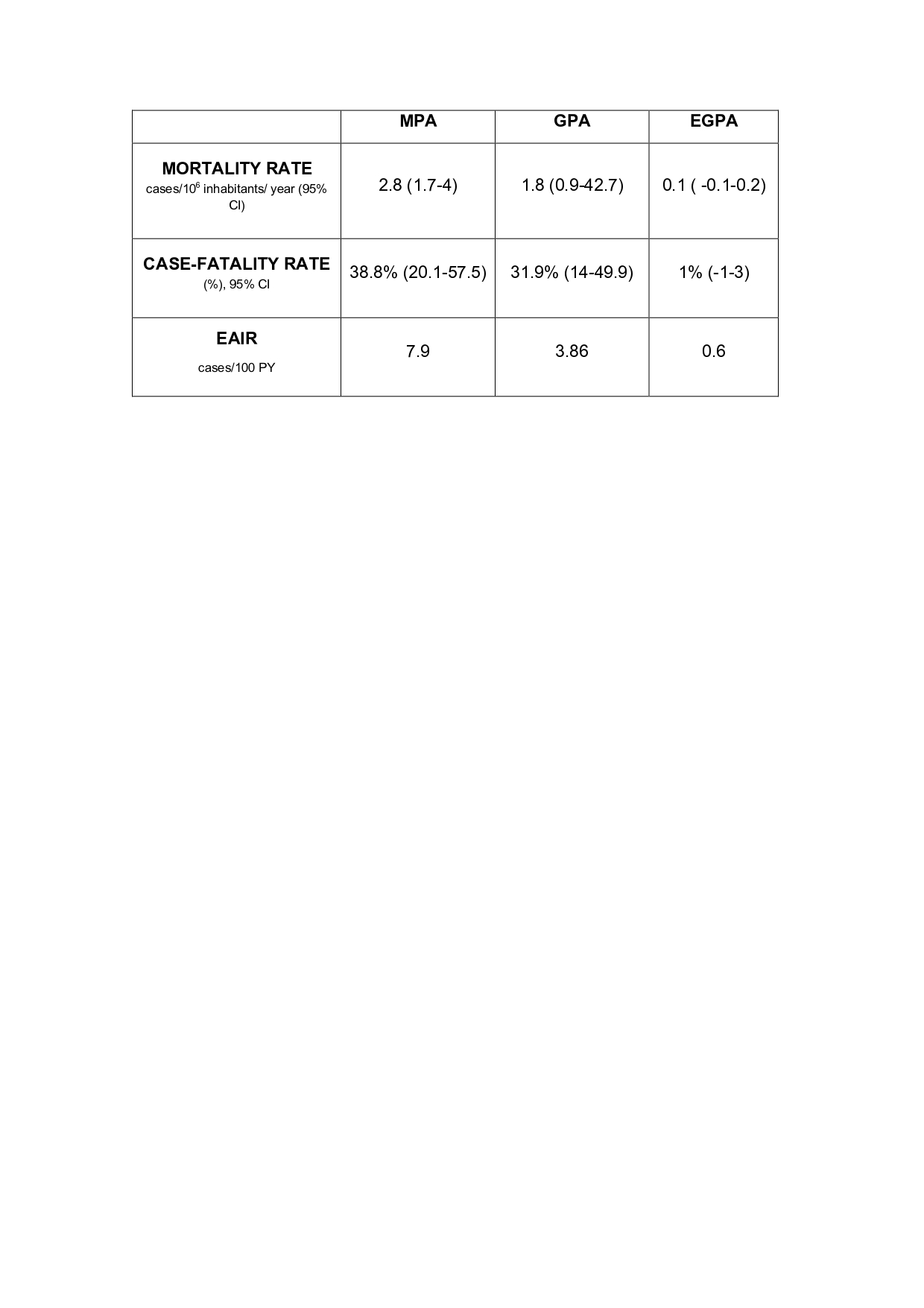 TABLE. Comparison of Mortality and Case-Fatality Rates by ANCA Vasculitis Subtypes.
TABLE. Comparison of Mortality and Case-Fatality Rates by ANCA Vasculitis Subtypes.
.jpg) FIGURE. Main causes of death by ANCA Vasculitis Subtypes.
FIGURE. Main causes of death by ANCA Vasculitis Subtypes.
To cite this abstract in AMA style:
Benavides Villanueva F, Calvo-Río V, Prieto-Peña D, Renuncio-García M, Martin-Gutierrez A, Sanchez-Lopez A, Poo-fernandez C, Escagedo-Cagigas C, Rodríguez-Vidriales m, Blanco R. Mortality in Anca-associated Vasculitis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/mortality-in-anca-associated-vasculitis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/mortality-in-anca-associated-vasculitis/