Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: The Intermittent and Constant Osteoarthritis Pain (ICOAP) measure was developed to evaluate the OA pain experience, independent of the effect of pain on physical activity. ICOAP has been shown to be reliable, valid and responsive to treatment in knee OA. This study sought to establish for ICOAP the Minimal Clinically Important Difference (MCID) for improvement and worsening, and the Patient Acceptable Symptom State (PASS).
Methods: In subjects with painful knee OA, the ICOAP was administered twice by telephone, two-weeks apart. The ICOAP is comprised of two subscales (constant and intermittent pain); the total score (range 0-100) is the sum of subscale scores, with higher scores indicating worse pain. At both time points, participants were asked to report their knee pain in the past 48 hours and the acceptability of their current knee pain state (acceptable or unacceptable). At second interview, participants were asked to report the degree to which their knee pain had changed (5-point scale from much worse to much better). MCID was calculated as the mean absolute change in ICOAP scores (Time 2 – Time 1) for those who reported ‘slightly better’ or ‘slightly worse’ versus ‘no change’. PASS was defined as the threshold ICOAP score at or above which participants considered their pain as ‘unacceptable’. Logistic regression was used to assess the ability of ICOAP change scores to predict reported improvement or worsening, and the relationship between scores and pain state acceptability.
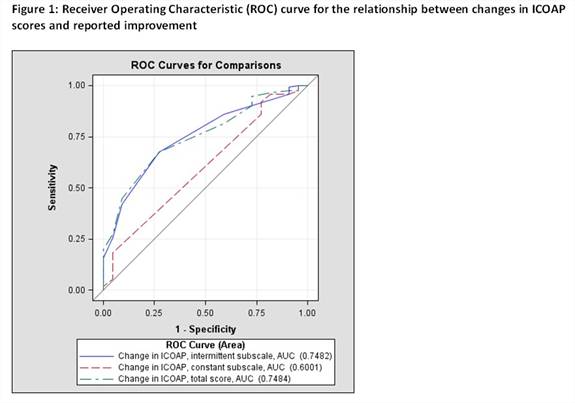
Results: 136 participants completed the study; 66 (54%) were female with a mean age of 73.9 years (SD 9.5). Median ICOAP constant, intermittent and total scores were 0/100 (range 0-90), 37.5 (0-87.5) and 25 (4.6-88.6), respectively, at Time 1 and 0 (0-95), 37.5 (0-95.8), and 23.9 (4.6-95.5) at Time 2. ‘Slight improvement’ was associated with a mean decrease of 2 and 7 points for the ICOAP constant and intermittent scales, respectively, while ‘slight worsening’ was associated with a mean increase of 4 points for both scales. The threshold ICOAP subscale scores associated with an unacceptable symptom state were: 20/100 (constant pain); 40/100 (intermittent pain); and 30/100 (total score). Changes in ICOAP subscale and total scores had good discriminative validity for self-reported improvement versus no change/worsening (Figure 1; AUC = 0.60-0.75) and for reported worsening (AUC 0.73-0.82). Absolute ICOAP scores were highly predictive of the acceptability of symptom state (AUC 0.71-0.84).
Conclusion: In an observational cohort, we determined the MCID and PASS for ICOAP total and subscale scores. These findings will assist clinicians and researchers in interpreting the clinical meaning of ICOAP scores for pain in knee OA. Future work will determine whether ICOAP MCID values differ across settings, including with clinical interventions.
Disclosure:
Z. A. Liu,
None;
T. Kendzerska,
None;
J. Elkayam,
None;
S. Ram,
None;
G. A. Hawker,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/minimal-clinically-important-difference-and-patient-acceptable-symptom-state-for-the-oarsi-omeract-intermittent-and-constant-oa-pain-icoap-measure/