Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Methotrexate (MTX) holds a unique place in the management of rheumatoid arthritis (RA) given its favorable balance between efficacy and safety. However, conflicting data still suggest a potential risk of MTX-induced long-term liver fibrosis. The fibrosis-4 (FIB-4) index was originally proposed as a simple and non-invasive marker of liver fibrosis in HIV/HCV co-infection. In patients with RA, FIB-4 values have been correlated to the amount of histologic liver lesions, suggesting that this index may be a valuable marker to diagnose liver disease in RA patients. Our objective was to estimate the amount of scarring in the liver with the FIB-4 index in RA patients on maintenance therapy with MTX.
Methods: We performed a cross-sectional study including successive RA patients hospitalized in the Rheumatology department of Cochin Hospital for a 12-month period. Data on liver function, disease activity, hepatotoxic and cardiovascular risk factors were systematically collected. The FIB-4 index was calculated according the following formula: (age(years) ×AST(U/L)/platelet (PLT) (109/L) × √ALT(U/L)). Using a lower cutoff value of 1.45, a FIB-4 score < 1.45 had a negative predictive value of 90% for advanced fibrosis in the patient cohort in which this formula was first validated. In contrast, a FIB-4 >3.25 had a 97% specificity and a positive predictive value of 65% for advanced fibrosis.
Results: We included 170 patients with established RA: 141 (83%) were women, the mean age was 59±12 years and the mean disease duration was 15±11 years. Positive rheumatoid factors and anti-CCP antibodies were detected in 134 patients (79%). 102 patients (60%) were treated with methotrexate, with a mean dose of 10.0±8.4 mg/week, a mean treatment duration of 9.5±10.3 years and a cumulative dose of 5.3±5.1g. 23 patients (13.5%) received conventional synthetic disease modifying anti-rheumatic drugs (csDMARDs) other than MTX, 112 (66%) corticosteroids (99 with a dose < 10 mg/day) and 85 targeted biologic DMARDs (bDMARDs) (50%).
The mean FIB-4 value was 1.24±0.57, with 120 patients (71%) with value < 1.45, 49 (29%) with values ranging from 1.45 to 3.25 and a single patient with FIB-4 >3.25. The FIB-4 was low and not significantly different between patients receiving MTX, patients previously treated with MTX and patients never treated with MTX (median 1.1, 1.25 and 1.18, respectively, p=0.709). This result was not modified after adjustment on treatments with other csDMARDs, corticosteroids, and bDMARDs. No correlation was observed between FIB-4 values and the cumulative dose of MTX (r=0.09, p=0.271). The FIB-4 index was low and similar between patients receiving cumulative MTX doses < 5g, between 5 and 10g and 10g (Figure 1). The cumulative dose of MTX was not significantly higher in patients with a FIB-4 index >1.45 (median cumulative MTX dose 5.5g vs. 3.5g, p=0.302).
No association was detected between the FIB-4 index and parameters of disease activity (DAS28, ESR and CRP levels), the body mass index, traditional cardiovascular risk factors and metabolic syndrome.
Conclusion: RA patients with long-term maintenance MTX therapy have low FIB-4 values suggesting that MTX is not associated with an increased risk of advanced liver fibrosis.
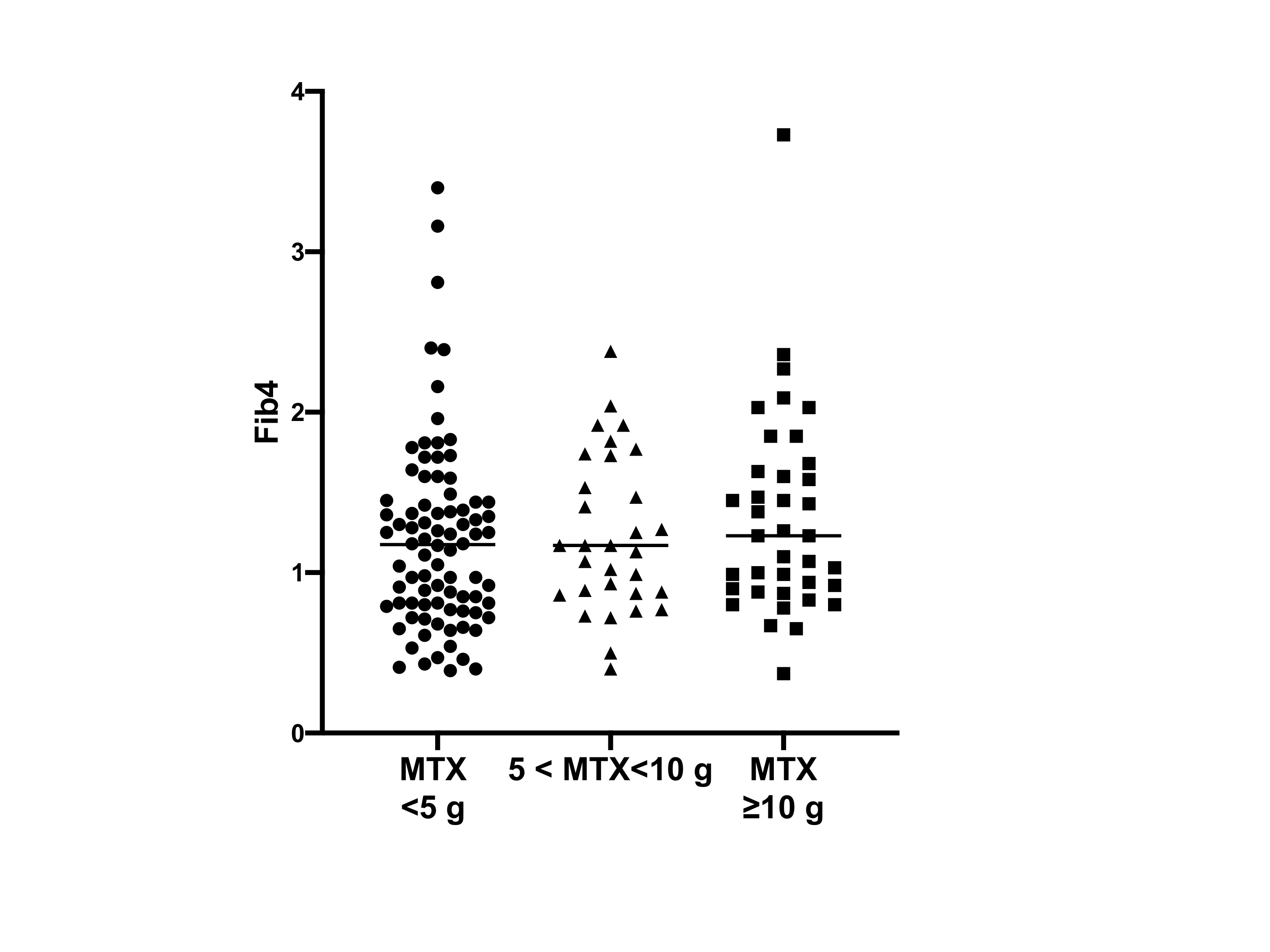 Figure 1: Fibrosis-4 index according to the cumulative dose of methotrexate in patients with rheumatoid arthritis
Figure 1: Fibrosis-4 index according to the cumulative dose of methotrexate in patients with rheumatoid arthritis
To cite this abstract in AMA style:
Avouac J, Degrave R, Vergneault H, Allanore Y. Methotrexate Therapy Is Not Associated with an Increased Risk of Liver Fibrosis Assessed by the Fibrosis-4 Index [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/methotrexate-therapy-is-not-associated-with-an-increased-risk-of-liver-fibrosis-assessed-by-the-fibrosis-4-index/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/methotrexate-therapy-is-not-associated-with-an-increased-risk-of-liver-fibrosis-assessed-by-the-fibrosis-4-index/