Session Information
Date: Tuesday, October 28, 2025
Title: (2547–2566) ARP Posters I
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Uncontrolled gout (UG) is defined by persistently high sUA levels, despite the use of oral urate lowering treatments (ULT), resulting in gout-related manifestations. Current ACR guidelines recommend a treat-to-target approach with routine sUA monitoring and a sUA goal of < 6mg/dL with the use of ULTs. The aim of this study was to assess current UG management, treatment practices and perceptions among rheumatologists.
Methods: A retrospective medical chart audit was conducted in the US from March to June 2024, via a web-enabled case report form, among board-certified rheumatologists with ≥3 years of clinical practice experience recruited via a panel. Respondents were required to have treated ≥25 patients with gout and ≥10 patients with UG in the last year. Data were abstracted from medical records of patients who met the following criteria: Diagnosed with UG, experienced gout related symptoms in the last year and have a sUA >6 mg/dL. Key variables included patient demographics, treatment history, adherence and healthcare resource utilization. Rheumatologists also completed an online survey related to their perceptions of UG management using a 1-7 Likert scale. Scores ≥6 indicates higher/strong level of satisfaction or agreement, while scores < 6 indicates the contrary.
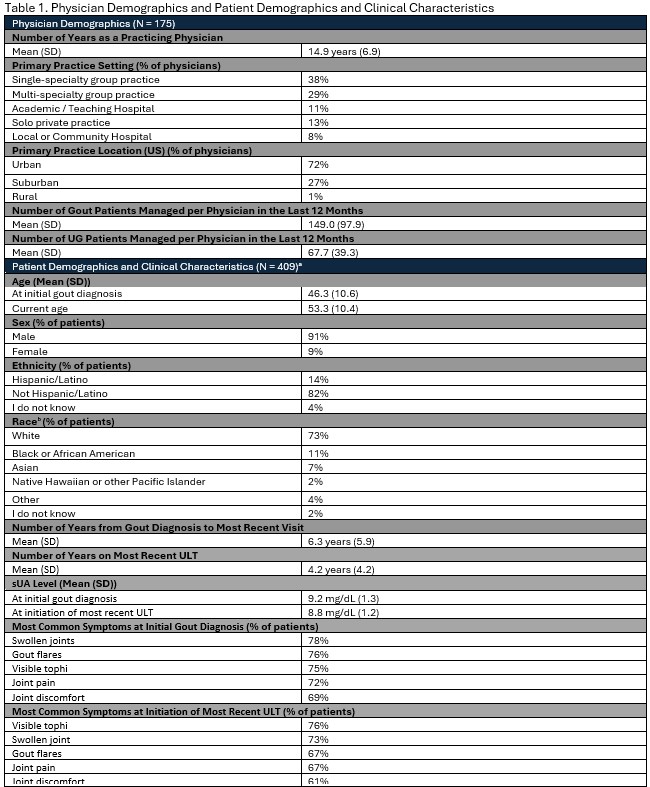
Results: A total of 175 rheumatologists abstracted 409 records of patients with UG (Table 1). In the past year, on average (SD), physicians managed 149 (98) patients with gout, with 68 (39) classified as having UG. Most commonly reported comorbidities were renal impairment (71%), hypertension (47%) and obesity (36%). At most recent visit, most patients had visible tophi (90%; 39% considered very severe), gout flares (58%; 61% very severe), swollen joints (47%; 54% very severe), joint pain (47%; 48% very severe) and joint discomfort (47%; 49% very severe). Rheumatologists reported measuring sUA at every visit in a majority (90%) of their patients, with patients having on average (SD), 3.9 (2.6) routine visits in the past year. As of the most recent visit, mean (SD) sUA level was 8.2 mg/dL (1.3). Clinical manifestations and sUA drive treatment choice, with treatments chosen due to sUA levels (75%), frequency of gout flares (57%) and severity of gout flares (42%) (Figure 2).
Patients with UG most recently received allopurinol (72%), with a median (IQR) dose of 300 mg/day (300-400) and 32% prescribed >300 mg/day. Other patients most recently received febuxostat (24%), colchicine (18%) and pegloticase (4%). Only 25% of patients were considered adherent (i.e., taking medication >75% of the time) with lack of compliance, most commonly attributed to forgetfulness (68%), lack of health literacy around medication (46%) or gout (35%). Rheumatologists were extremely satisfied with allopurinol in 60% of their patients, febuxostat in 50%, pegloticase in 22%. About 37% of rheumatologists indicated that unmet needs exist in current management of UG and 31% believed their patients are impacted by the burden of current gout treatments (Figure 3).
Conclusion: This study highlights the challenges rheumatologists face in managing UG and unmet needs in gout treatments as evidenced by high sUA levels, frequent flares and tophi presence and low adherence rates to current ULTs.
 * UG is defined as the following: a) Inadequate control of symptoms and failure to normalize sUA with xanthine oxidase inhibitors, or where these drugs are contraindicated for the patient b) Serum uric acid (sUA) > 6 mg/dL c) A history of symptomatic gout (> 2 gout flares within 12 months, and/or presence of > 1 gout tophus, and/or current diagnosis of gouty arthritis)
* UG is defined as the following: a) Inadequate control of symptoms and failure to normalize sUA with xanthine oxidase inhibitors, or where these drugs are contraindicated for the patient b) Serum uric acid (sUA) > 6 mg/dL c) A history of symptomatic gout (> 2 gout flares within 12 months, and/or presence of > 1 gout tophus, and/or current diagnosis of gouty arthritis)
.jpg)
.jpg)
To cite this abstract in AMA style:
Choi H, Kragh N, Athavale A, Desai B, Gulaid A, Oladapo A, Smith B, Saag K. Management of Uncontrolled Gout Among Rheumatologists: Findings from a Medical Chart Audit [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/management-of-uncontrolled-gout-among-rheumatologists-findings-from-a-medical-chart-audit/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/management-of-uncontrolled-gout-among-rheumatologists-findings-from-a-medical-chart-audit/