Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: To assess the experience, views and opinions of rheumatology providers at Veterans Affairs (VA) facilities about rheumatic disease healthcare issues during the COVID-19 pandemic.
Methods: We used the Qualtrics™ survey to perform an anonymized cross-sectional survey of all VA rheumatology providers, who were members of the VA Rheumatology Consortium, a volunteer organization of VA rheumatologists. Non-responders received reminders to complete the survey from April 16 to May 18, 2020. We assessed provider experience, views and opinions about various COVID-19 issues and resilience.
Results: Of the 153 eligible VA rheumatologists, 103 (67%) completed the survey. Potential participants were slightly older (16% vs. 11% were ≥65 yrs) and more likely to be male compared to the survey responders (45% vs. 38%).
Established patients. Most/majority of rheumatologists considered that the following conditions were appropriate for telephone follow-up visits: gout, osteoporosis, polymyalgia rheumatica, stable rheumatoid arthritis, stable spondyloarthritis, and osteoarthritis (Figure 1). One-third or more rheumatologists considered it appropriate to have a video based VA video connect (VVC) visit for local musculoskeletal conditions, tendinitis, rheumatoid arthritis with active medication (DMARD/biologic) changes and patients with stable lupus, scleroderma or vasculitis; 53% preferred an in-person for people with lupus, scleroderma, vasculitis with immunosuppressive or glucocorticoid dose changes (Figure 1).
Most/majority of the responders were somewhat or very comfortable with technology for providing healthcare to established patients during COVID-19 pandemic using: (1) telephone, 87%; (2) VA video connect (VVC), 64%; and (3) in-person visits, 54% (Figure 2). A smaller proportion were comfortable with technology providing healthcare to new clinic patients (Figure 2).
High provider resilience was independently associated with significantly higher odds ratio (OR) of more comfort with technology for telephone (OR, 3.1 (95% CI, 1.1-9.7)) and VVC visits for new patients (OR, 4.7 (95% CI, 1.4-15.7)), with no difference for in-person visits (OR, 1.8 (95% CI, 0.7-5.0)).
Live vaccine. Most responders would not hold hydroxychloroquine (95%) or sulfasalazine for a live COVID-19 vaccine (74%). A majority would hold methotrexate or leflunomide (66%) and glucocorticoids of 20 mg/day or higher (52%) for 2 weeks or less (Figure 3); and would hold non-TNF biologics (76%), anti TNF-biologics (85%), Janus-kinase inhibitors (78%), anti IL-17/23 biologics (82%), belimumab (77%)immunosuppressive drugs such as azathioprine (64%), for 3-8 weeks (Figure 3).
Killed vaccine. A majority of responders (50% or higher) would not withhold these drugs for a killed COVID-19 vaccine; another 25% would hold them off for < 2 weeks (Figure 3).
Conclusion: A better understanding of COVID-19 rheumatic disease healthcare issues using a health-system approach can inform improve the care of Veterans with rheumatic disease and their providers.
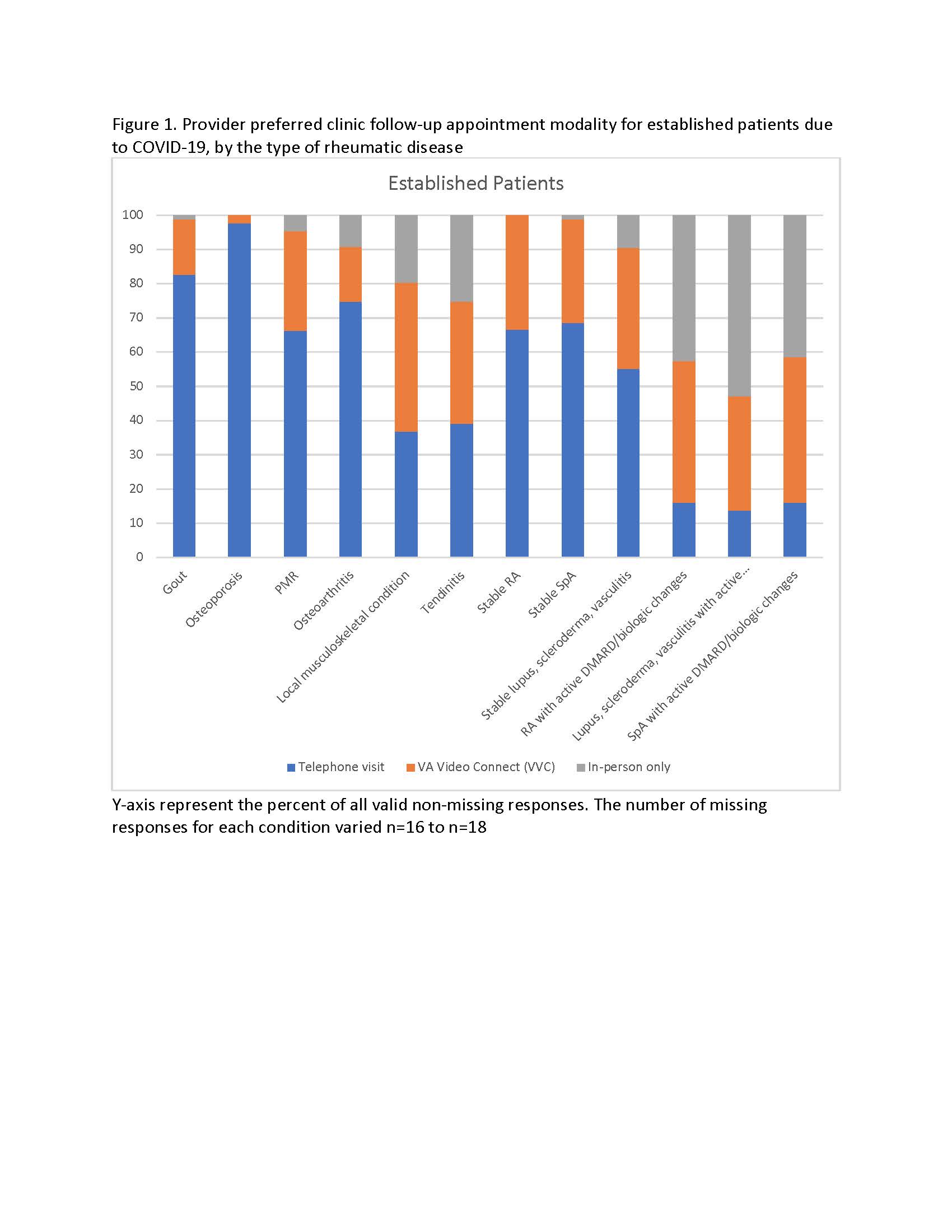 Figure 1. Provider preferred clinic follow-up appointment modality for established patients due to COVID-19, by the type of rheumatic disease Figure 1 legend. Y-axis represent the percent of all valid non-missing responses. The number of missing responses for each condition varied n=16 to n=18. VA telehealth includes 3 modalities: (1) telephone care; (2) a video-based VA video connect (VVC) visit with the healthcare provider, usually with the patient at home; and (3) clinical video telehealth (CVT) visits with a facilitator, usually with a facilitator (nurse, technician, primary care provider) assisting patient examination at a healthcare facility close to patient’s home. Due to limited relevance of CVT facilitator during the COVID-19 pandemic, choices offered were telephone care, video-based VVC or in-person visit
Figure 1. Provider preferred clinic follow-up appointment modality for established patients due to COVID-19, by the type of rheumatic disease Figure 1 legend. Y-axis represent the percent of all valid non-missing responses. The number of missing responses for each condition varied n=16 to n=18. VA telehealth includes 3 modalities: (1) telephone care; (2) a video-based VA video connect (VVC) visit with the healthcare provider, usually with the patient at home; and (3) clinical video telehealth (CVT) visits with a facilitator, usually with a facilitator (nurse, technician, primary care provider) assisting patient examination at a healthcare facility close to patient’s home. Due to limited relevance of CVT facilitator during the COVID-19 pandemic, choices offered were telephone care, video-based VVC or in-person visit
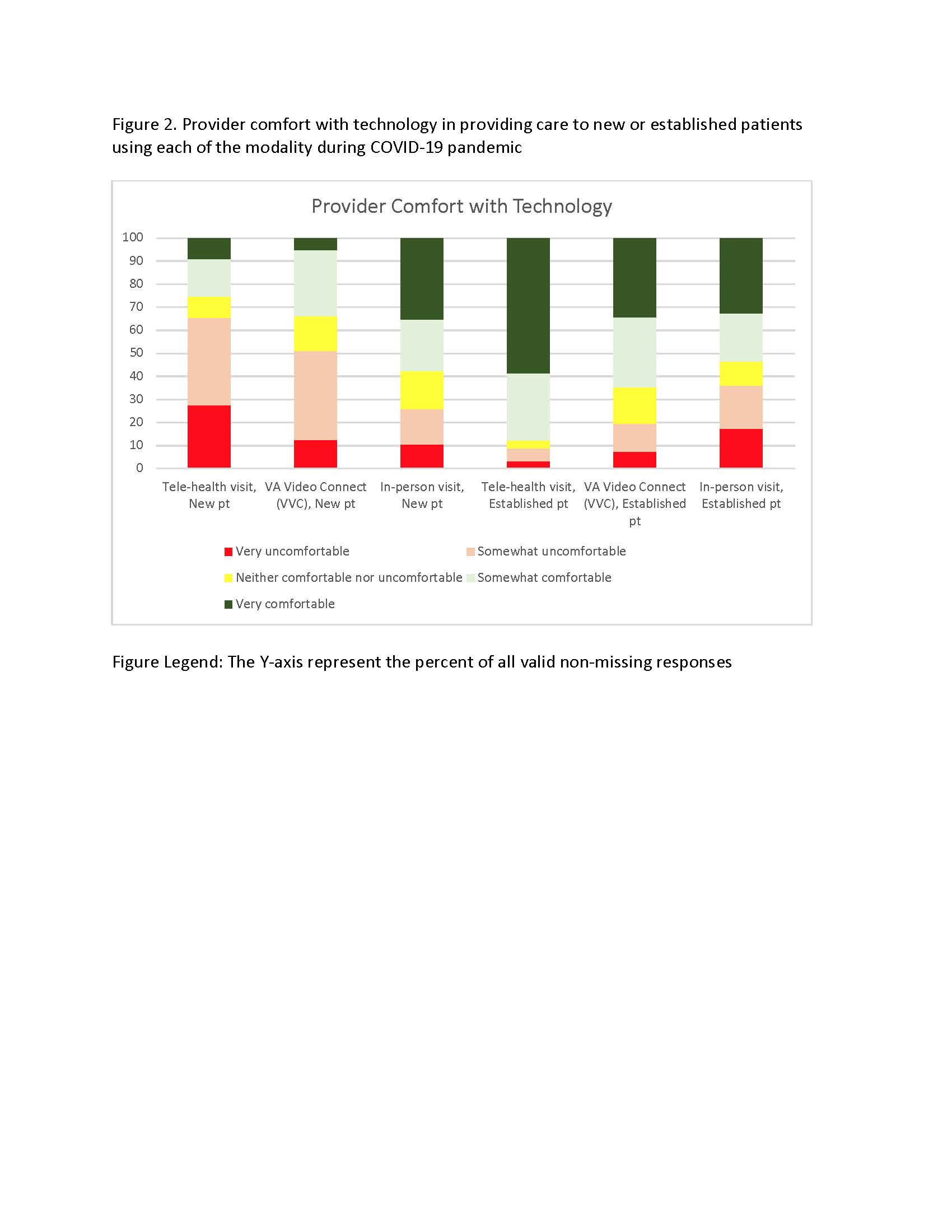 Figure 2. Provider comfort with technology in providing care to new or established patients using each of the modality during COVID-19 pandemic Figure Legend: The Y-axis represent the percent of all valid non-missing responses
Figure 2. Provider comfort with technology in providing care to new or established patients using each of the modality during COVID-19 pandemic Figure Legend: The Y-axis represent the percent of all valid non-missing responses
 Figure 3. Provider opinion on period of withholding of treatments for rheumatic diseases for administering a potential COVID-19 live (3A) or killed (3B) vaccine Figure Legend: The Y-axis represent the percent of all valid non-missing responses
Figure 3. Provider opinion on period of withholding of treatments for rheumatic diseases for administering a potential COVID-19 live (3A) or killed (3B) vaccine Figure Legend: The Y-axis represent the percent of all valid non-missing responses
To cite this abstract in AMA style:
Singh J, Richards J, Chang E, Joseph A, Ng B. Management of Rheumatic Diseases During COVID-19: A National Veterans Affairs Survey of Rheumatologists [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/management-of-rheumatic-diseases-during-covid-19-a-national-veterans-affairs-survey-of-rheumatologists/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/management-of-rheumatic-diseases-during-covid-19-a-national-veterans-affairs-survey-of-rheumatologists/