Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Sarcoidosis is a systemic inflammatory disease characterized by granuloma formation. Clinical manifestations are heterogenous, but most commonly affect the pulmonary system. Current biomarkers lack accuracy to predict disease severity and clinical outcomes. Prior studies have demonstrated a relationship between peripheral blood lymphopenia and disease severity. This study explores the use of lymphopenia in a predominantly African American cohort at the time of diagnosis as a marker for disease severity.
Methods: Patients who were diagnosed with sarcoidosis via biopsy at a tertiary academic care center between 2011-2020 were included in the study. Eligible subjects had a baseline lymphocyte count within 3 months of diagnosis and received follow up care at this institution. Peripheral lymphopenia was defined as lymphocyte count less than or equal to 1,500 cells/uL. Outcome measures included clinical symptoms, treatment, and pulmonary function tests at time of diagnosis at time of diagnosis and follow up. Data were analyzed using Fisher’s exact test, independent samples T test, or Mann-Whitney test. Cox proportional hazard was applied to change in forced vital capacity (FVC) over time.
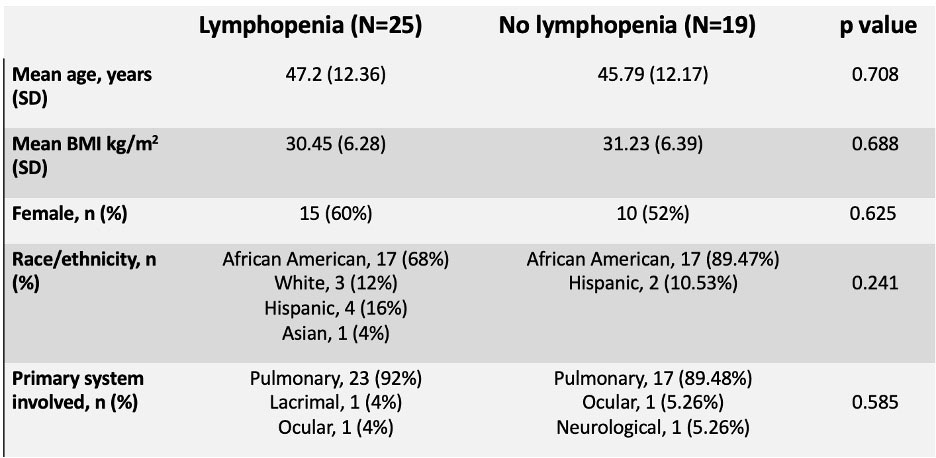
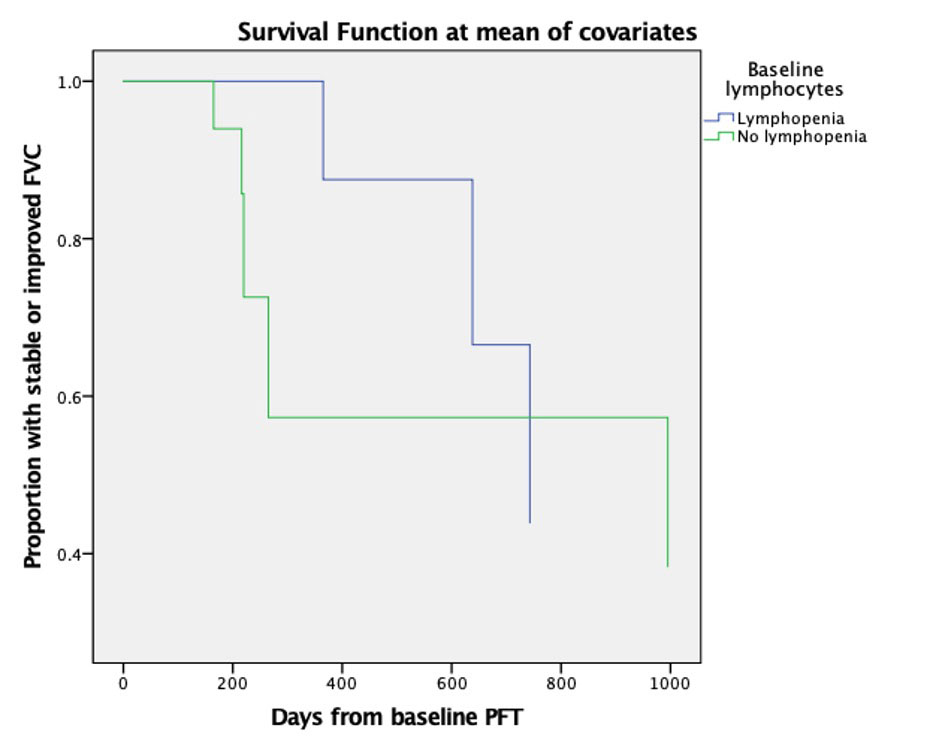
Results: 44 patients were included in the study. 56.8% of patients demonstrated lymphopenia at the time of diagnosis. There was no statistically difference in age, BMI, race/ethnicity, or organ involvement between the lymphopenia (L) and no lymphopenia (NL) groups. There was no significant difference in treatment initiation at diagnosis (p = 0.610, 80% and 78.94%, L vs NL respectively). Treatments included corticosteroids, methotrexate, or hydroxychloroquine. There was no significant difference in the presence of abnormal pulmonary function test (PFT) (p=0.465). PFTs were interpreted based on standard guidelines. There was no statistically significant difference in the baseline percent predicted forced vital capacity (FVC) (p = 0.361, 91.06% and 96.99%, L vs NL groups, respectively). Cox proportional hazardwas calculated to evaluate deterioration in FVC over time. Deterioration was defined as any subsequent decrease in FVC from baseline. Patients with baseline lymphopenia showed deterioration in FVC later in their disease course.
Conclusion: In this study the majority of patients had pulmonary involvement. This cohort is unique as patients were identified early in their disease course and were treatment naïve when the lymphocyte count was measured. This study supports the high prevalence of baseline lymphopenia that has been found in prior studies. This study did not show any significant differences in need for treatment initiation or PFTs results in patients based on the presence of lymphopenia, which may be due to the limited sample size of the study. A prior study in Caucasian patients showed sarcoidosis patients with lymphopenia diagnosis were more likely to develop a severe disease course. However, in our cohort of predominantly African American patients, we found that patients with baseline lymphopenia experienced worsened FVC later in their disease course compared to those without lymphopenia. This finding can possibly be attributed to racial disparities in presentation and treatment of sarcoidosis.
To cite this abstract in AMA style:
Manansala M, Ascoli C, Sweiss N. Lymphopenia as a Marker of Disease Activity and Severity in Sarcoidosis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/lymphopenia-as-a-marker-of-disease-activity-and-severity-in-sarcoidosis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/lymphopenia-as-a-marker-of-disease-activity-and-severity-in-sarcoidosis/