Session Information
Date: Sunday, October 26, 2025
Title: (0593–0640) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: No studies have directly examined the link between 25-hydroxyvitamin D [25(OH)D] and cardiovascular outcomes in SLE. This study aimed to assess this association, hypothesizing that low 25(OH)D levels correlate with increased mortality and cardiovascular event risk in SLE.
Methods: Our longitudinal cohort measured 25(OH)D levels at quarterly clinic visits from 2009 onwards. Patients were categorized based on their first measured, mean, and most recent 25(OH)D levels (the last two measures reflecting supplementation). The “most recent 25(OH)D” was defined as the 25(OH)D level measured at the most recent past visit. The first prospective analysis examined monthly follow-up data, categorizing by 25(OH)D levels and assessing cardiovascular events (CVE) or mortality using pooled logistic regression. For the analysis using mean 25(OH)D levels, the mean 25(OH) vitamin D in previous visits was the mean 25(OH)D level from all visits prior to that month. The second lifetime analysis evaluated the association between initial 25(OH)D levels and a patient’s lifetime cardiovascular event history, adjusting for confounders with a Cox Proportional Hazards model. This approach included events that might occur before cohort entry.
Results: The study analyzed a cohort of 1,792 SLE patients, primarily female (92%), White (48%), and African American (40%), with a mean age of 42 years. In the prospective analysis, cardiovascular events (CVE; defined as stroke, myocardial infarction (MI), and angina/bypass) were assessed over 11,302 person-years of follow-up, with 67 events recorded. Patients with 25(OH)D levels below 20 ng/mL had the highest mortality and CVE rates (Table 1). Only initial 25(OH)D levels were significantly associated with mortality and cardiovascular risk, while mean and recent levels were not (Table 2). Compared to patients with levels of 30-39 ng/mL, those with levels below 20 ng/mL had: higher mortality risk (HR: 2.05, 95% CI: 1.19–3.54, p = 0.0095); higher risk of CVE (HR: 1.74, 95% CI: 1.20–2.54, p = 0.0038); increased MI risk (HR: 2.42, 95% CI: 1.12–5.24, p = 0.025); but no significant association with stroke (HR: 1.41, 95% CI: 0.90–2.20, p = 0.14).In the second (lifetime) analysis (Table 3), the analysis included more CVE than the prospective analysis (261 stroke/MI/angina; 229 stroke or MI; 176 stroke; 76 MI). A U-shaped relationship was observed, with both low ( < 20 ng/mL) and high (≥50 ng/mL) 25(OH)D levels linked to an increased risk of myocardial infarction. Using mean 25(OH)D levels in the model for mortality (assuming the log-rate of mortality declines in a linear way), the slope was significant (p=0.0002). The odds ratio was 0.72 for each 10 unit increase in mean 25(OH)D level (i.e., a 28% decline in mortality per 10 unit increase in 25(OH)D levels).
Conclusion: An initial 25(OH)D level below 20 ng/mL led to a significantly increased risk of mortality and cardiovascular events (but not stroke) in SLE. The U-shaped association with MI, found in the lifetime analysis, suggests both deficient and high 25(OH)D levels increase the risk of myocardial infarction. Analysis of mean 25(OH)D levels (which represent routine supplementation) found a 28% decline in mortality per 10 unit increase in 25(OH)D levels.
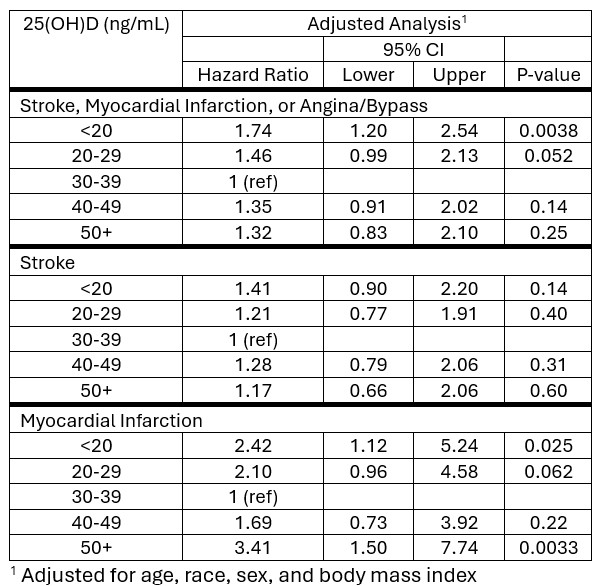 Table 1: Rates of Cardiovascular events (Myocardial Infarction, Stroke, Angina, or Bypass), by Demographic variables and 25(OH)D levels
Table 1: Rates of Cardiovascular events (Myocardial Infarction, Stroke, Angina, or Bypass), by Demographic variables and 25(OH)D levels
.jpg) Table 2: Prospective Analysis of 25(OH)D Levels and Mortality, Combined Cardiovascular Events, Stroke Alone and Myocardial Infarction Alone.
Table 2: Prospective Analysis of 25(OH)D Levels and Mortality, Combined Cardiovascular Events, Stroke Alone and Myocardial Infarction Alone.
.jpg) Table 3: Lifetime Relationship Between 25(OH)D Levels Measured at the First Cohort Visit and Risk of Stroke, Myocardial Infarction, or Angina/Bypass; Stroke Alone; and Myocardial Infarction Alone
Table 3: Lifetime Relationship Between 25(OH)D Levels Measured at the First Cohort Visit and Risk of Stroke, Myocardial Infarction, or Angina/Bypass; Stroke Alone; and Myocardial Infarction Alone
To cite this abstract in AMA style:
Assawasaksakul T, Fava A, Goldman D, Magder L, Petri M. Low 25-hydroxyvitamin D Levels are Associated with Higher Mortality and More Cardiovascular Events in Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/low-25-hydroxyvitamin-d-levels-are-associated-with-higher-mortality-and-more-cardiovascular-events-in-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/low-25-hydroxyvitamin-d-levels-are-associated-with-higher-mortality-and-more-cardiovascular-events-in-systemic-lupus-erythematosus/