Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: In Canada, adolescents with JIA and jSLE transfer from pediatric to adult care around age 18. This vulnerable transition period is associated with an increased risk of poor symptom and disease control, morbidity, and even mortality. These risks necessitate efforts be made to minimize the potential of loss to follow-up (LFU) at the time of transfer. Despite significant advances in research and models of transition to adult care, there has been a dearth of LFU data worldwide since the reporting of LFU rates (50%) from one Canadian centre in 2010. Despite identified challenges in determining LFU rates, we aimed to i) determine LFU rates of patients seen in a multidisciplinary transition program after transfer to adult care, and ii) describe characteristics of patients who were and were not LFU.
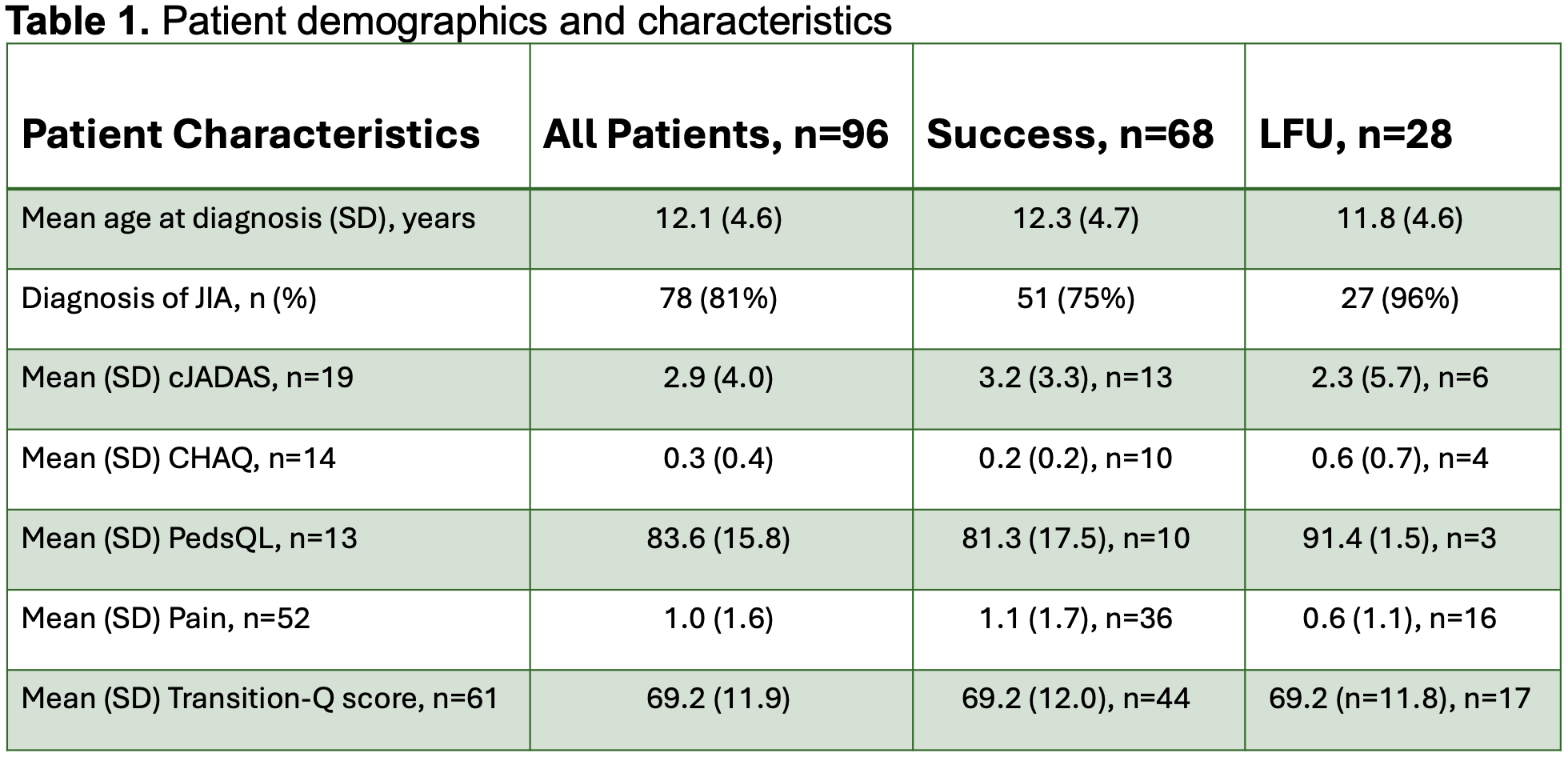
Methods: We performed a retrospective review of patients diagnosed with JIA or jSLE followed in the McMaster Children’s Hospital multidisciplinary rheumatology transition clinic and enrolled in a prospective, observational transition study. The clinic is staffed by pediatric and adult rheumatologists, nurses, an Advanced Physiotherapist Practitioner (APP), and a Child Life Specialist. Patients who did not attend their first or attended their first but not their second adult appointment were considered LFU. Patients seen at least twice in adult rheumatology or discharged after their first appointment were considered successful transfers. Patient demographics, disease characteristics (cJADAS 0-30, CHAQ 0-3, QoL 0-100, and pain 0-10) and transition readiness (Transition-Q, max 100) scores were recorded. Continuous variables were described using means and standard deviations, and categorical variables using frequencies and proportions. Differences in disease characteristics and Transition-Q scores were analyzed using unpaired t-tests.
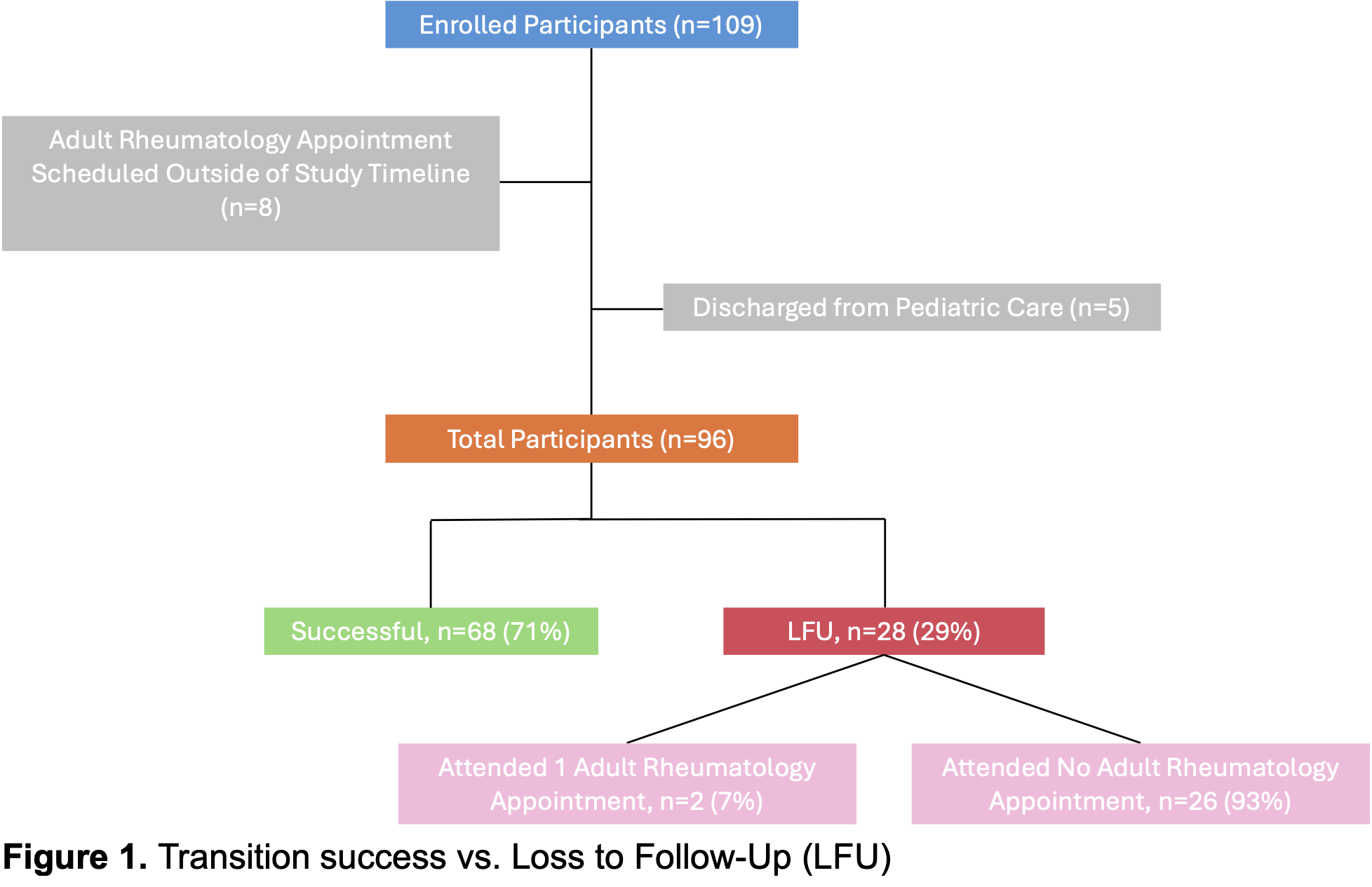
Results: Ninety-six participants (n=65 female, 31 male) were included, of whom 71% successfully transferred to adult care (71% female) and 29% were LFU (61% female) (Figure 1). Patients took, on average, 21.3 months (12.4 SD) to successfully transfer from their last Transition Clinic appointment to their second adult rheumatology visit. Of those LFU, 93% never saw their adult rheumatologist. Those who were LFU had lower disease activity and pain scores, greater quality of life scores, and similar Transition-Q scores than those who were not LFU but the differences in disease characteristics and transition readiness were not statistically signfiicant (Table 1).
Conclusion: Integrating coordinated transfer of care processes from a multidisciplinary pediatric transition clinic resulted in lower LFU rates (29%) than previously reported (50%). Improved LFU rates may lead to improved long-term outcomes of patients with JIA or jSLE. While incomplete clinical data limited our results, those who were LFU appeared to be doing well compared to those who were not. However, differences in disease characteristics and Transition-Q scores were not significantly different between those who were and were not LFU. Future analyses will explore potential LFU predictors (e.g., disease status, parental involvement) and determine the impact of a transition coach intervention on rates of LFU.
To cite this abstract in AMA style:
Heera S, Sholdice M, Cellucci T, Garner S, Heale L, Matsos M, BEATTIE K, Batthish M. Loss to Follow up After Transfer from Pediatric to Adult Care in Patients with JIA or jSLE [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/loss-to-follow-up-after-transfer-from-pediatric-to-adult-care-in-patients-with-jia-or-jsle/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/loss-to-follow-up-after-transfer-from-pediatric-to-adult-care-in-patients-with-jia-or-jsle/