Session Information
Title: Rheumatoid Arthritis - Clinical Aspects: Novel Biomarkers and Other Measurements of Disease Activity
Session Type: Abstract Submissions (ACR)
Background/Purpose: Patient-reported outcome measures are important tools that assess the impact of disease on patients’ lives; in RA, patient-reported physical function is especially relevant. In contrast to legacy measures such as the Health Assessment Questionnaire (HAQ) or Short Form 36 Health Survey (SF-36), the Patient-Reported Outcome Measurement Information System (PROMIS) scales are brief and intended to address psychometric flaws in earlier measures such as ceiling effects. However, use of PROMIS in clinical practice has been limited. The current study evaluates the ceiling and floor effects of the PROMIS Physical Function short form 10a (PROMIS-PF10a) relative to the HAQ, and compares the construct validity of these measures to a commonly used measure of disease activity (Clinical Disease Activity Index, CDAI), among patients with RA in an ethnically diverse urban clinic.
Methods: We abstracted demographic and clinical data from the electronic health record (EHR) of patients from a university-based rheumatology clinic. Eligible patients had 2 ICD-9 codes for RA between February 2013 and March 2014, had completed PROMIS-PF10a and HAQ, and had CDAI scores recorded by a clinician. We characterized score distributions for PROMIS T-scores and HAQ, including percent of patients with minimum and maximum possible scores. Construct validity was evaluated by examining the matrix of correlation coefficients (Pearson’s r) among PROMIS-PF10a, HAQ and CDAI.
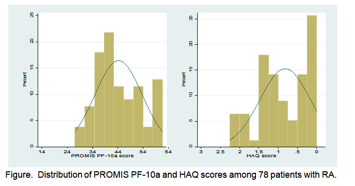
Results: Analyses included 78 patients. 78% were female, mean age was 57.0± 14.4 years, 59% were Caucasian, 15% Hispanic/Latino, and 10% Asian. 82% were RF or CCP positive, 51% had erosive disease and mean disease duration was 12± 11 years. The mean PROMIS-PF10a score was 44.3; the mean HAQ score was 0.82. The distribution of PROMIS-PF10a scores more closely approximated a normal distribution (Figure), and had a lower proportion of scores at the ceiling (Table). There was a statistically significant correlation between PROMIS-PF10a and HAQ scores of r = -0.61, and a modest significant correlation between PROMIS-PF10a and CDAI scores of r = -0.48. The relationship between HAQ and CDAI was not statistically significant (r = 0.19).
Conclusion: In this ethnically diverse RA clinic population, the shorter PROMIS-PF10a had a distribution closer to normal with less ceiling effect, which enables better discrimination at higher levels of functioning. PROMIS-PF10a also had a higher correlation with CDAI scores than HAQ. Further studies are needed to understand the relative responsiveness of changes in PROMIS physical function scores compared to legacy measures.
|
Table. Score Characteristics and Floor/Ceiling Effects for PROMIS-PF10a and HAQ. |
||||||
|
MEASURE |
Scores |
Floor (poorest function) |
Ceiling (best function) |
|||
|
|
Mean± SD |
Median |
Min |
Max |
N (%) |
N (%) |
|
PROMIS-PF10a |
44.3± 9.3 |
41.4 |
27.1 |
61.7 |
0 |
10 (12.8%) |
|
HAQ |
0.82± 0.66 |
0.88 |
0 |
2.25 |
0 |
15 (19.2%) |
|
Higher PROMIS-PF10a scores reflect better function while higher HAQ reflects poorer function. Normalized PROMIS-PF10a scores can range from 14.1-61.7. A score of 50 represents average function in a healthy individual; each 10-point decrement represents one standard deviation from this norm. HAQ scores range from 0-3. A score of 0 represents no limitation in functioning. |
||||||
Disclosure:
E. R. Wahl,
None;
A. J. Gross,
None;
R. K. Chaganti,
None;
L. S. Gensler,
UCB,
5,
AbbVie,
5,
Celgene Corporation,
9;
V. Chernitskiy,
None;
L. Trupin,
None;
P. P. Katz,
None;
J. Yazdany,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/less-is-more-the-shorter-physical-function-measure-promis-pf10a-outperforms-haq-in-an-ethnically-diverse-urban-rheumatoid-arthritis-clinic-population/