Session Information
Date: Tuesday, November 9, 2021
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster II (1862–1888)
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: Deficiency of adenosine deaminase 2 (DADA2) leads to a broad phenotype that in some resembles polyarteritis nodosa with fever and rash, but in others is characterised by stroke or immunodeficiency. Small, medium and large vessel vasculitis has been reported. In contrast, plasma ADA2 activity is elevated in inflammatory conditions including systemic lupus erythematosus and systemic juvenile idiopathic arthritis with macrophage activation syndrome. The role of ADA2 and how its deficiency associates with the vasculitides is not yet understood. Using a well-characterised large vessel vasculitis cohort we sought to establish the potential role of ADA2 activity.
Methods: ADA2 activity was measured in adults with Takayasu arteritis (TA), large vessel giant cell arteritis (LV-GCA), intracranial vasculitis (IV) and healthy control (HC) subjects (Table 1), using a coupled spectrophotometric assay as previously described. Plasma from 11 patients with genotyped DADA2 and 10 patients heterozygous for pathogenic variants in ADA2 were used to define thresholds for deficiency and carrier status respectively (DADA2 activity 0 – 0.90 U/L, ADA2 carrier activity 2.02 – 10.62 U/L). Activity levels above the upper limit of normal (ULN) were defined as >99th percentile of the HC activity (30.3 U/L). To assess potential associations with TA disease status, ADA2 was measured prospectively in matched active and remission samples.
TA disease activity was determined as active, grumbling or stable using clinical and radiological features, physician impression, CRP, ESR and Indian Takayasu clinical Activity Score (ITAS).
Median values are presented with differences between groups analysed using non-parametric tests, P< 0.05 was considered significant.
Results: No patients were found to have ADA2 deficiency while 7 subjects had activity within the carrier range (1 HC (1.9%), 5 TA (3.7%), 1 LV-GCA (2.3%)). Compared to HC levels (17.43 [14.11 – 20.78] U/L), activity in the TA group was significantly increased (TA 19.68U/L, p= 0.0061), while LV-GCA and IV were not significantly different (Figure 2). In 20 cases activity exceeded the upper limit of normal; 16 TA (11.9%, p=0.044; 4 active, 2 grumbling, 10 stable) and 4 LV-GCA (9.1%, ns). In TA, there was a positive correlation between ADA2 activity and ESR (Spearman R = 0.2863, p=0.0009) but not with CRP or ITAS score.
Subgroup analysis revealed that ADA2 activity was most prominently elevated in the stable group relative to HCs (TA stable 20.54 U/L [8.08 – 48.66], median +17.8%, p= 0.0006), but not with active or grumbling disease. Consistent with this, prospective analysis demonstrated a significant increase in ADA2 activity in remission vs active disease (p=0.024), with activity increasing in 18 (62%) patients achieving remission (Figure 3).
Conclusion: There were no cases of ADA2 deficiency in this cohort. Consistent with other inflammatory conditions, ADA2 activity was elevated in TA compared to HC subjects. Surprisingly, increased ADA2 activity was linked to stable TA in both cross-sectional and prospective analyses. This may suggest a potential role of ADA2 enzyme activity in vascular repair and regrowth – possibly tying in with known elevated levels of ADA2 activity in growing children
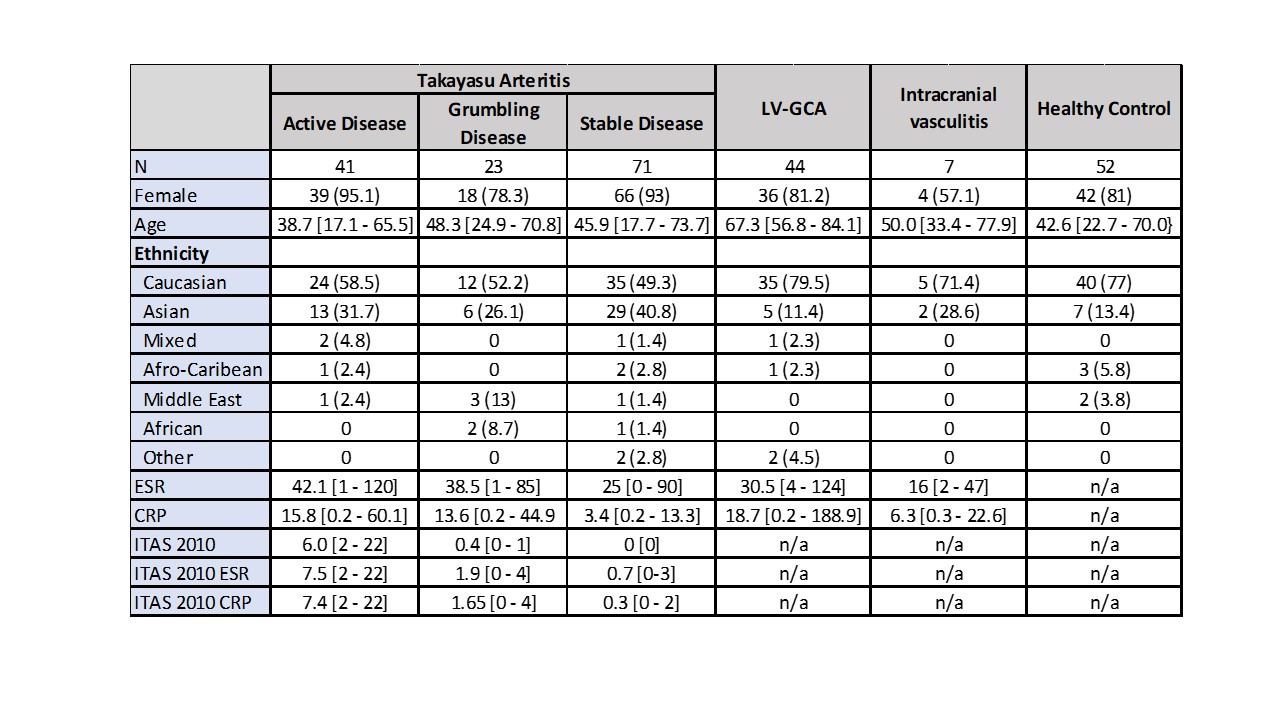 Table 1 – Demographic data. LV-GCA – large vessel giant cell arteritis. ITAS – Indian Takayasu clinical Activity Score. ESR – Erythrocyte sedimentation rate. CRP – C-reactive protein.
Table 1 – Demographic data. LV-GCA – large vessel giant cell arteritis. ITAS – Indian Takayasu clinical Activity Score. ESR – Erythrocyte sedimentation rate. CRP – C-reactive protein.
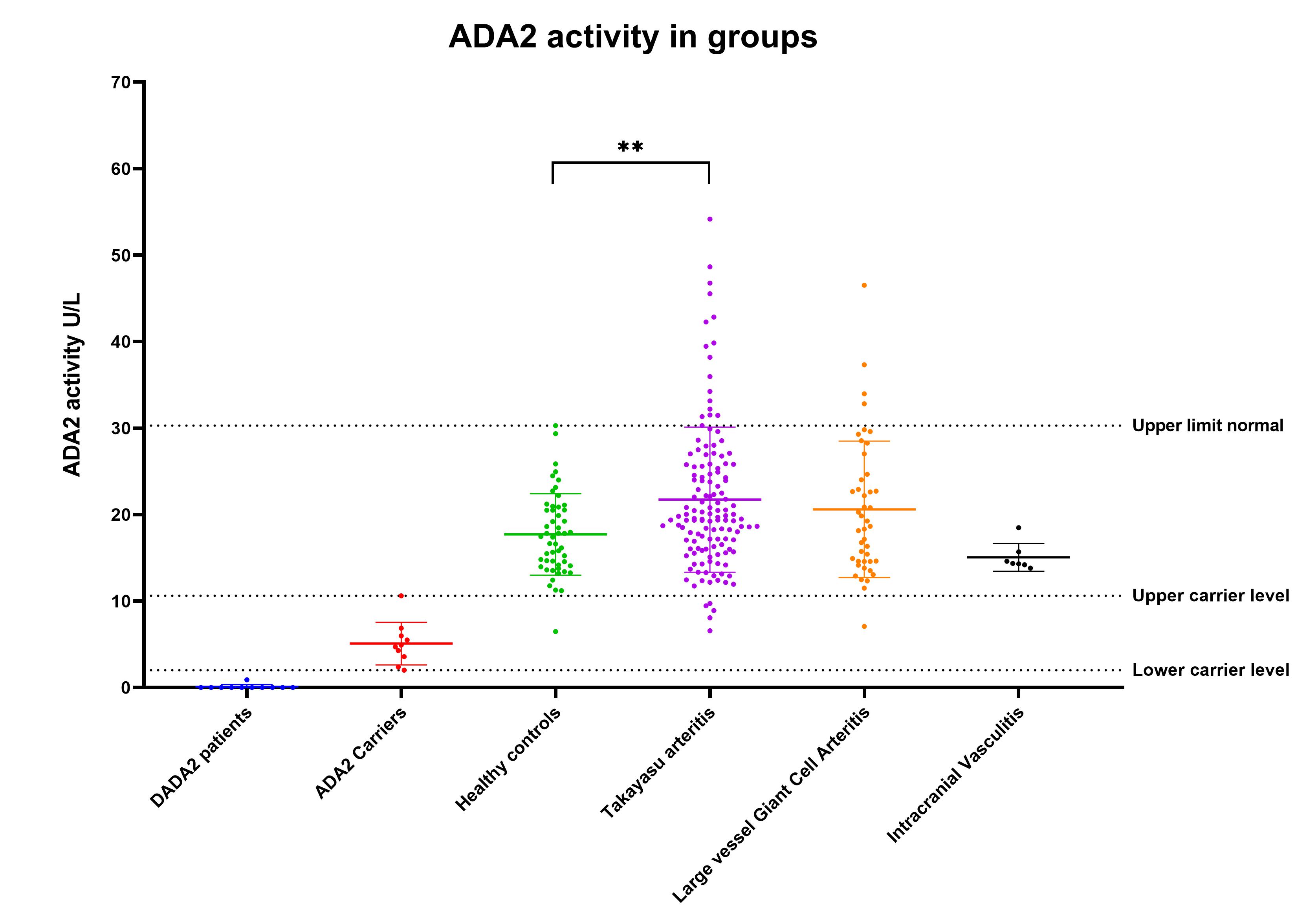
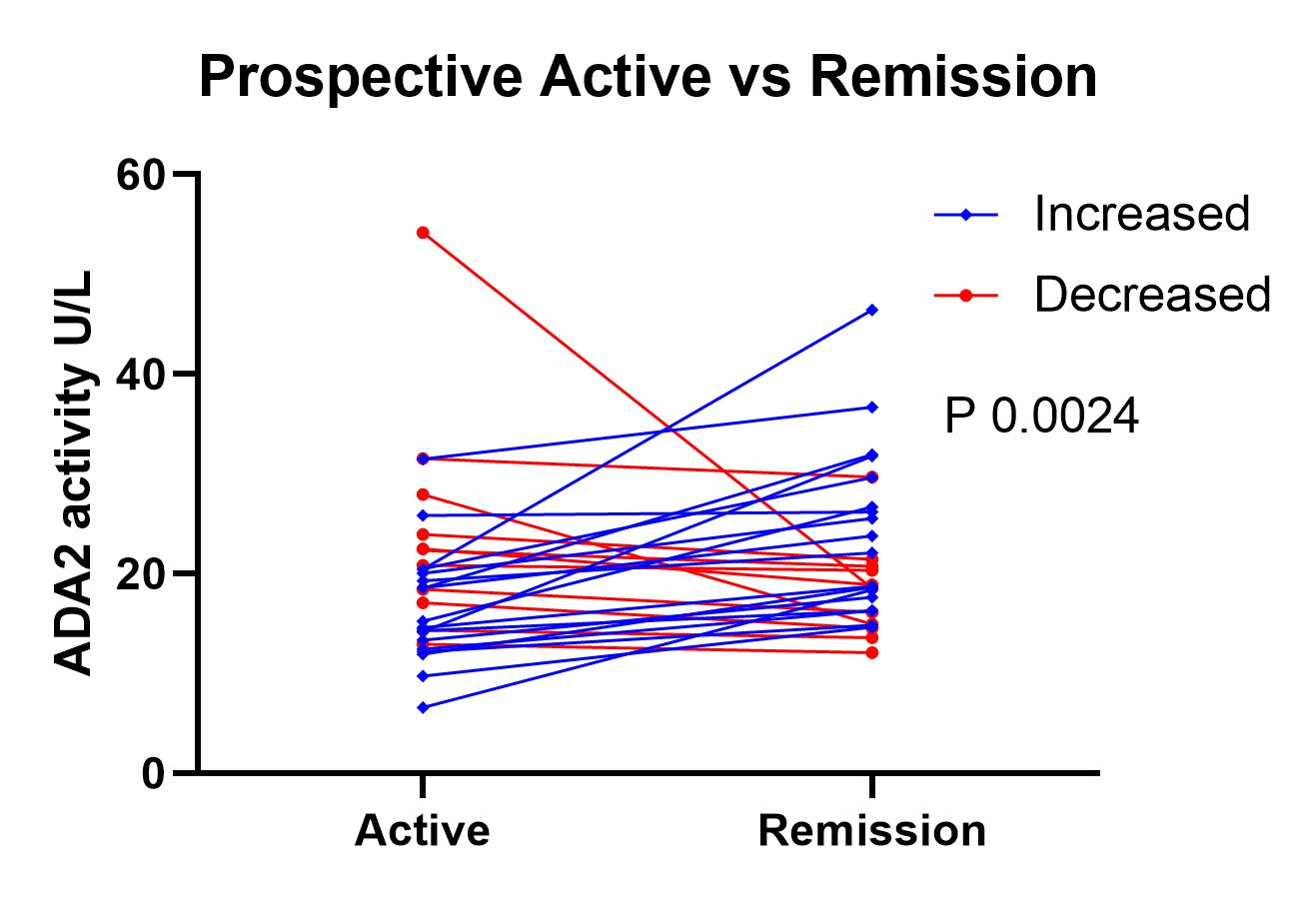 Figure 3 – ADA2 activity in prospective active and remission samples. Increased – ADA2 activity higher in remission vs active. Decreased – ADA2 activity lower in remission vs active.
Figure 3 – ADA2 activity in prospective active and remission samples. Increased – ADA2 activity higher in remission vs active. Decreased – ADA2 activity lower in remission vs active.
To cite this abstract in AMA style:
Porter A, Maughan R, Pericleous C, Kiprianos A, Jee H, Lee P, Youngstein T, Mason J. Investigating Adenosine Deaminase 2 Activity in Large Vessel Vasculitis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/investigating-adenosine-deaminase-2-activity-in-large-vessel-vasculitis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/investigating-adenosine-deaminase-2-activity-in-large-vessel-vasculitis/