Session Information
Date: Monday, November 14, 2022
Title: Abstracts: Epidemiology and Public Health II: COVID, Infection and Pregnancy Outcomes
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Patients with autoimmune diseases (AIDs) display a risk of invasive fungal diseases (IFDs), because of the underlying disease or treatments used. Our objective was to describe the characteristics of IFDs in patients with AID and factors associated with mortality.
Methods: We analysed IFD cases included into a prospective multicenter registry conducted by the French national reference center for invasive mycoses and antifungals. We performed clustering after multiple correspondence analysis and a multivariable Cox model for factors associated with mortality.
Results: From 2012 to 2018, 552 individuals with IFD and AID were included, mainly with Pneumocystis jirovecii pneumonia (PCP) (n=229, 41.5%), fungemia (n=168, 30.4%) and invasive aspergillosis (n=84, 15.2%) (other IFD: n=58; multiple IFD: n=13). Rheumatoid arthritis (RA) and systemic vasculitis were the most frequent underlying AIDs in patients with PCP (respectively n=55 and n=42) and invasive aspergillosis (n=15 and n=14). Inflammatory bowel diseases (IBD) were predominant in fungemia (n=36). At IFD diagnosis, 346 (62.7%) patients received glucocorticoids (GCs) and 321 (58.2%) received immunosuppressive agents, mainly methotrexate (n=113), azathioprine (n=38) and cyclophosphamide (n=27). Mortality at 90 days was 34.5% (174/504), and was higher in invasive aspergillosis (31/81, 38.3%) and fungemia (72/148, 48.7%) compared to PCP (54/207, 26.1%) (p< 0.001) (figure 1). Fungemia (hazard ratio 2.4, 95% confidence interval 1.6-3.5, compared with PCP), advanced age (HR 2.1, 95% CI 1.3-3.2, for age ≥70 years compared with age < 55), cirrhosis (HR 3.7, 95% CI 2.1-6.4), and use of high-dose GCs ( > 0.3 mg/kg/day for > 1 month at IFD diagnosis) (HR 1.7, 95% CI 1.2-2.3) were independently associated with higher mortality. Clustering analysis identified three clusters: Cluster 1 consisted mainly of patients with PCP, IFD occurred 1 year after AID diagnosis in median, and almost all received high doses of GCs. Cluster 2 included mostly patients with RA, less frequently receiving GCs, and IFD occurred long after AID diagnosis (median 6 years). Cluster 3 included almost exclusively fungemia, occurring long after AID diagnosis (median 8 years). Cluster 2 (24.4%) displayed a lower mortality than the other two (cluster 1: 39.5%; cluster 3: 40.5%; p = 0.002). PCP (n=239) mostly occurred early after AID diagnosis (median 2 years, interquartile range 0-11) except for cases with RA (9 years, IQR 3-18). CD4+ T cells were measured within 3 months of PCP diagnosis for 78 patients (32.6%): median level was 472.5/mm3 (IQR 198-858), 49.6% (IQR 36.8-65.3) and CD4/CD8 ratio 2.2 (IQR 1.3-4.3). Among cases of fungemia, patients with IBD had an improved survival (HR 0.19, 95% CI 0.07-0.52).
Conclusion: IFDs are associated with a high mortality in patients with AID. PCP is the main IFD in this population and occurs primarily in patients with RA. Fungemia (apart for patients with IBD), high-dose GCs, cirrhosis and older age are associated with poor survival. PCP occurs usually early after AID onset except in cases of RA. CD4 T cell lymphopenia, mostly absent in cases of PCP, poorly predicts the risk of PCP in patients with AID.
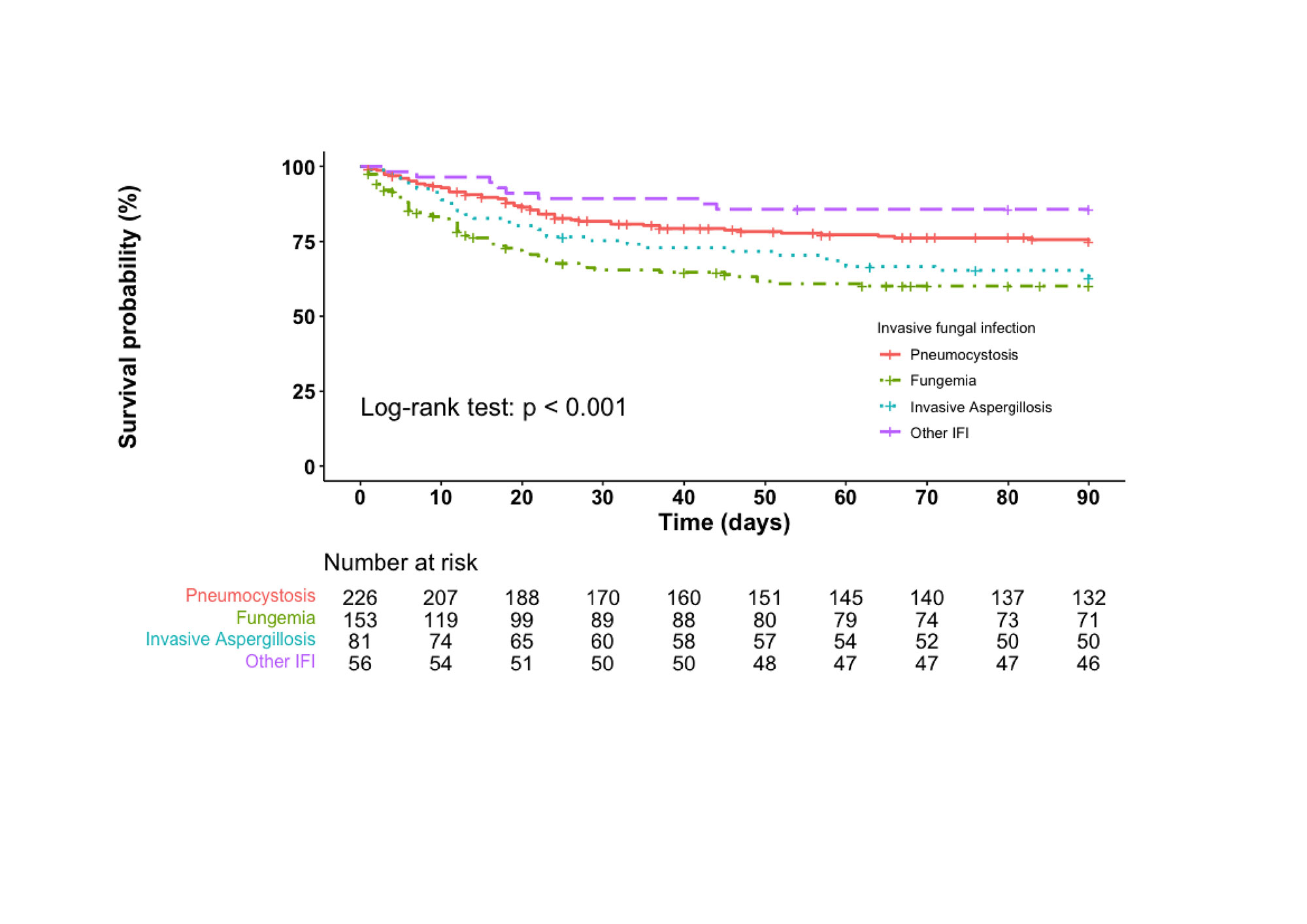
Legend: patients with multiple IFDs were not included in the analysis; 23 participants (including 21 dead and 2 lost to follow-up) were censored before date of diagnosis and were not included in the analysis
To cite this abstract in AMA style:
Galmiche S, Thoreau B, Bretagne S, Alanio A, Paugam A, Bru V, Cassaing S, Gangneux J, Guégan H, Favennec L, Minoza A, Morio F, Bonhomme J, Desoubeaux G, Eloy O, Hasseine L, Sasso M, Millon L, Bellanger A, Poirier P, Moniot M, Chouaki T, Huguenin A, Dalle F, Bouteille B, Nicolas M, Desbois-Nogard N, Bougnoux M, Danion F, Poindron V, Néel A, Boukris-Sitbon K, Lanternier F, Terrier B. Invasive Fungal Diseases in Patients with Autoimmune Diseases: Prospective Data from a Nationwide French Registry [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/invasive-fungal-diseases-in-patients-with-autoimmune-diseases-prospective-data-from-a-nationwide-french-registry/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/invasive-fungal-diseases-in-patients-with-autoimmune-diseases-prospective-data-from-a-nationwide-french-registry/