Session Information
Date: Monday, October 22, 2018
Title: 4M091 ACR Abstract: Vasculitis–Non-ANCA-Assocd & Rel D/Os I: Population-Based Studies(1881–1886)
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Previous studies have implicated infections as a risk factor for giant cell arteritis (GCA). The purpose of this study was to investigate the association between occurrence of infections and the development of GCA.
Methods: Patients diagnosed with biopsy-proven giant GCA between 2000 and 2016 were identified through the database of the Department of Pathology in Skåne, the southernmost region in Sweden. For each GCA case, 10 controls were randomly selected from the background population matched for age, sex, and area of residence. The index date for the controls was the same as the diagnosis date of their respective cases. We identified all infection events diagnosed before the date of GCA diagnosis (and before index date for controls) between 1998 and 2016, using the Skåne Healthcare Register based on International Classification of Diseases -10thversion (ICD-10) codes. First, we calculated the odds ratio (OR) of being exposed to an infection in GCA cases vs controls. Second, we evaluated the type of infection closest to the biopsy-proven GCA diagnosis (or index date). Conditional logistic regression models were used to calculate OR and 95% confidence intervals (CI).
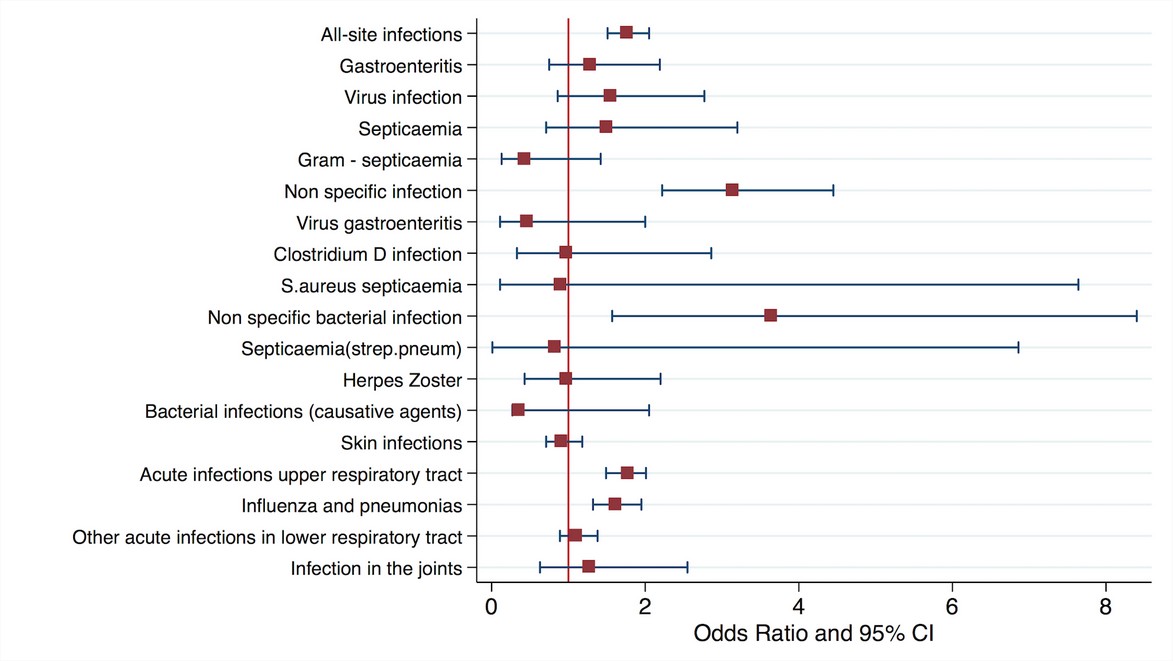
Results: 1005 patients with biopsy-proven GCA (714 women, 71%) and 10 050 controls were included in this study. In total, 476 unique infection diagnoses were assigned for GCA cases prior to the biopsy-proven diagnosis as compared to 3722 unique infections for controls. Infections were more common among patients going to develop GCA vs. controls (47% vs. 37%) yielding the OR of 1.76 (95% CI 1.51–2.05). The median time from the latest diagnosed infection to GCA diagnosis was 0.9 years (interquartile range (IQR) 0.1 – 3.5), whereas the corresponding median time for the controls was 2.2 years (IQR 0.8-4.7). Acute upper respiratory tract infections, pneumonia, influenza and non-specific bacterial infections, but not skin or gastrointestinal infections, were associated with increased probability for later biopsy-proven GCA (Figure 1).
Conclusion: Infections, especially upper respiratory tracts infections, pneumonias and influenza were associated with later development of biopsy-proven GCA. Our findings corroborate previous reports of an association between GCA and infectious pathogens of the respiratory tract. The observed associations with unspecified infections may partly reflect diagnostic uncertainty in the early phase of GCA.
Figure 1. Odds ratios for developing GCA associated with prior exposure to infection
To cite this abstract in AMA style:
Stamatis P, Turkiewicz A, Englund M, Jönsson G, Nilsson JÅ, Turesson C, Mohammad A. Infections Are Associated With Increased Risk of Giant Cell Arteritis – a Population-Based Case-Control Study From Southern Sweden [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/infections-are-associated-with-increased-risk-of-giant-cell-arteritis-a-population-based-case-control-study-from-southern-sweden/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/infections-are-associated-with-increased-risk-of-giant-cell-arteritis-a-population-based-case-control-study-from-southern-sweden/