Session Information
Date: Tuesday, October 28, 2025
Title: (2524–2546) Vasculitis – Non-ANCA-Associated & Related Disorders Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Giant cell arteritis (GCA), polymyalgia rheumatica (PMR), and ANCA-associated vasculitis (AAV) often require long-term glucocorticoid (GC) therapy, increasing the risk of infections, particularly in older adults with GCA and PMR. Biologics and small molecule therapies are increasingly used to reduce GC exposure but may also increase infection risk through immunosuppression. This systematic review aimed to evaluate the infection risk associated with these therapies along with concomitant GC treatment, as compared to GC treatment alone, in vasculitis clinical trials.
Methods: A comprehensive search of PubMed, Embase, and Cochrane, supplemented by ClinicalTrials.gov was conducted using terms related to GCA, PMR, AAV, biologic therapies (tocilizumab, sarilumab), small molecule therapies (upadacitinib, avacopan), glucocorticoids, and infections. We included randomized controlled trials (RCTs) published in English comparing biologics or small molecules with concomitant GC dosing (active intervention) compared to GC monotherapy (comparator), and reporting infection outcomes. Two independent reviewers screened titles and abstracts, conducted full-text reviews, and extracted data, including study characteristics, details about the intervention and comparator, mean cumulative glucocorticoid use, and overall infection outcomes. We calculated the difference in GC dose between the comparator and active intervention groups and relative risk of infection (active intervention versus comparator group).
Results: The initial search yielded 1,154 studies (Figure 1). We included 10 eligible phase II or III RCTs (1,487 patients total; Table 1). 4 trials evaluated tocilizumab, 2 sarilumab, 1 upadacitinib, and 3 avacopan among patients with GCA, PMR and AAV. All studies reported infection outcomes and included populations with mean age ≥50 years. Follow-up durations ranged from 6 to 18 months. Despite steroid-sparing protocols, cumulative GC use was greater than anticipated in both intervention and comparator groups. In most trials, the intervention group had lower cumulative GC exposure than the comparator group. The frequency of infection varied. When the comparators had much higher GC dosing than the active intervention, the RR for infection was either close to 1 or < 1 (Figure 2). When the active intervention GC dose was comparable to the comparator dose, the RR for infection was >1.
Conclusion: Although biologics and small molecules had lower overall cumulative GC exposure, they did not consistently lead to a lower infection risk. When GC exposure was notably higher in the comparator group, infection risk was lower in the intervention group suggesting a possible protective effect of reducing GC. However, when GC doses were more comparable between groups, infection risk was higher in the active intervention arm, likely due to the immunosuppressive effects of combining biologic and small molecules with GC. These findings emphasize the importance of carefully considering infection risk in the management of patients, particularly in older adult populations.
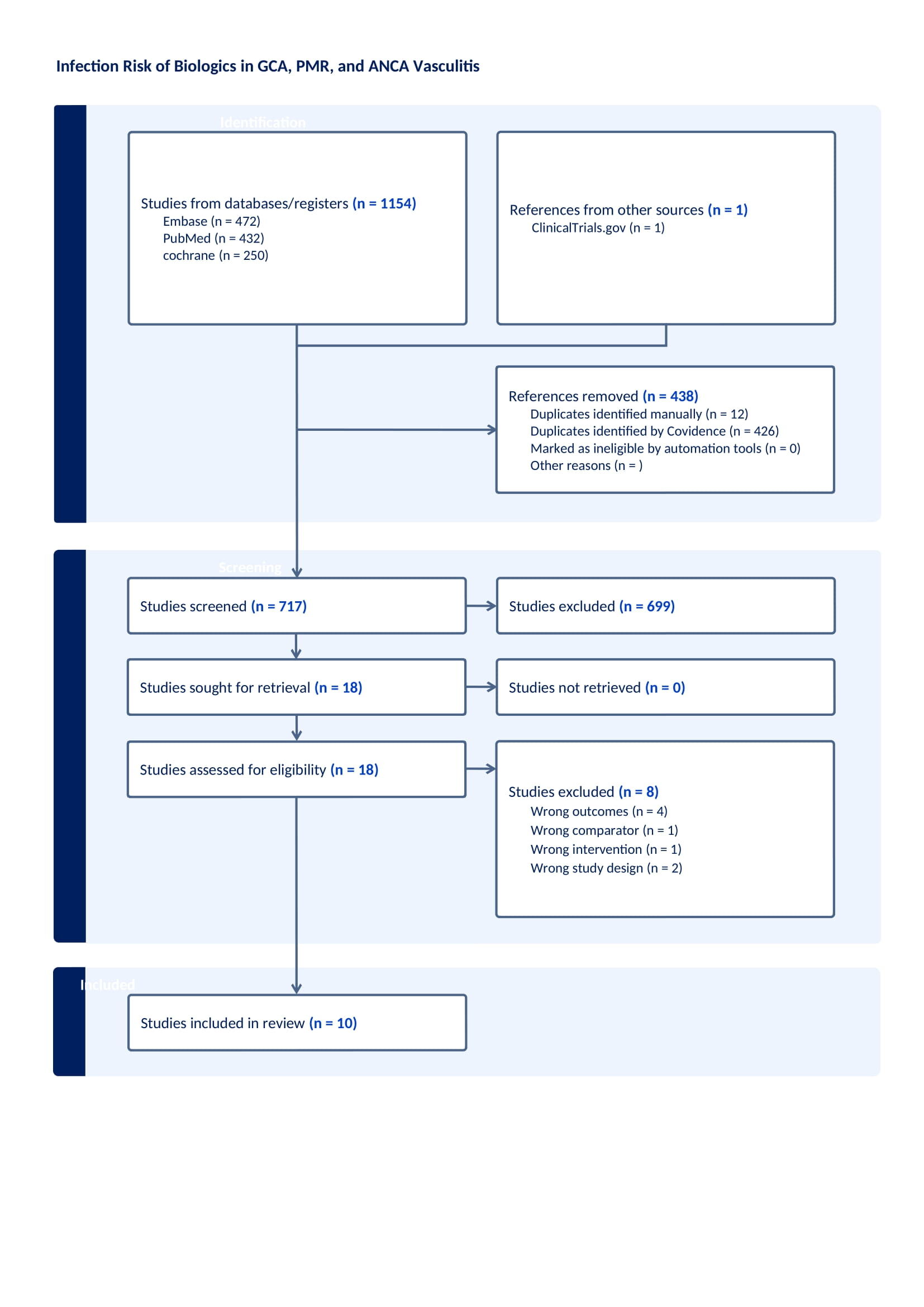 Figure 1. PRISMA flow diagram of study inclusion and exclusion
Figure 1. PRISMA flow diagram of study inclusion and exclusion
.jpg) Table 1: Characteristics of included studies, including glucocorticoid exposure and infection outcomes by intervention versus comparator arms
Table 1: Characteristics of included studies, including glucocorticoid exposure and infection outcomes by intervention versus comparator arms
.jpg) Figure 2: Infection risk ratios versus difference in mean cumulative glucocorticoid dosing between active intervention and comparator
Figure 2: Infection risk ratios versus difference in mean cumulative glucocorticoid dosing between active intervention and comparator
To cite this abstract in AMA style:
Sudireddy D, Leung B, Liew J, Neogi T, Felson D, LaValley M, Flynn D. Infection Risk Associated with Steroid-Sparing Therapies in GCA, PMR, and ANCA-Associated Vasculitis: A Systematic Review [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/infection-risk-associated-with-steroid-sparing-therapies-in-gca-pmr-and-anca-associated-vasculitis-a-systematic-review/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/infection-risk-associated-with-steroid-sparing-therapies-in-gca-pmr-and-anca-associated-vasculitis-a-systematic-review/