Session Information
Date: Saturday, November 12, 2022
Title: Vasculitis – ANCA-Associated Poster I: Epidemiology, Outcomes, and Classification
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Therapies for ANCA-associated vasculitis (AAV) have evolved over the last 3 decades. In light of new data on plasma exchange (PLEX) and glucocorticoid (GC) use, as well as recent approval of avacopan (AVP), various medical societies have updated their AAV management guidelines. Here, we explored practice patterns of induction therapy in severe AAV and ascertained differences in management by physician specialty, practice setting, and volume of AAV patients.
Methods: A 65-item anonymous research survey addressing physician/practice characteristics, AAV induction therapy approaches, prophylactic measures, and laboratory monitoring was sent to physicians by e-mail and social media platforms after IRB approval. Practice patterns within the last 5 years were examined based on physician specialty, practice setting, and volume of AAV patients. Descriptive statistics, chi-square, t-test, and Fisher’s exact were used as appropriate.
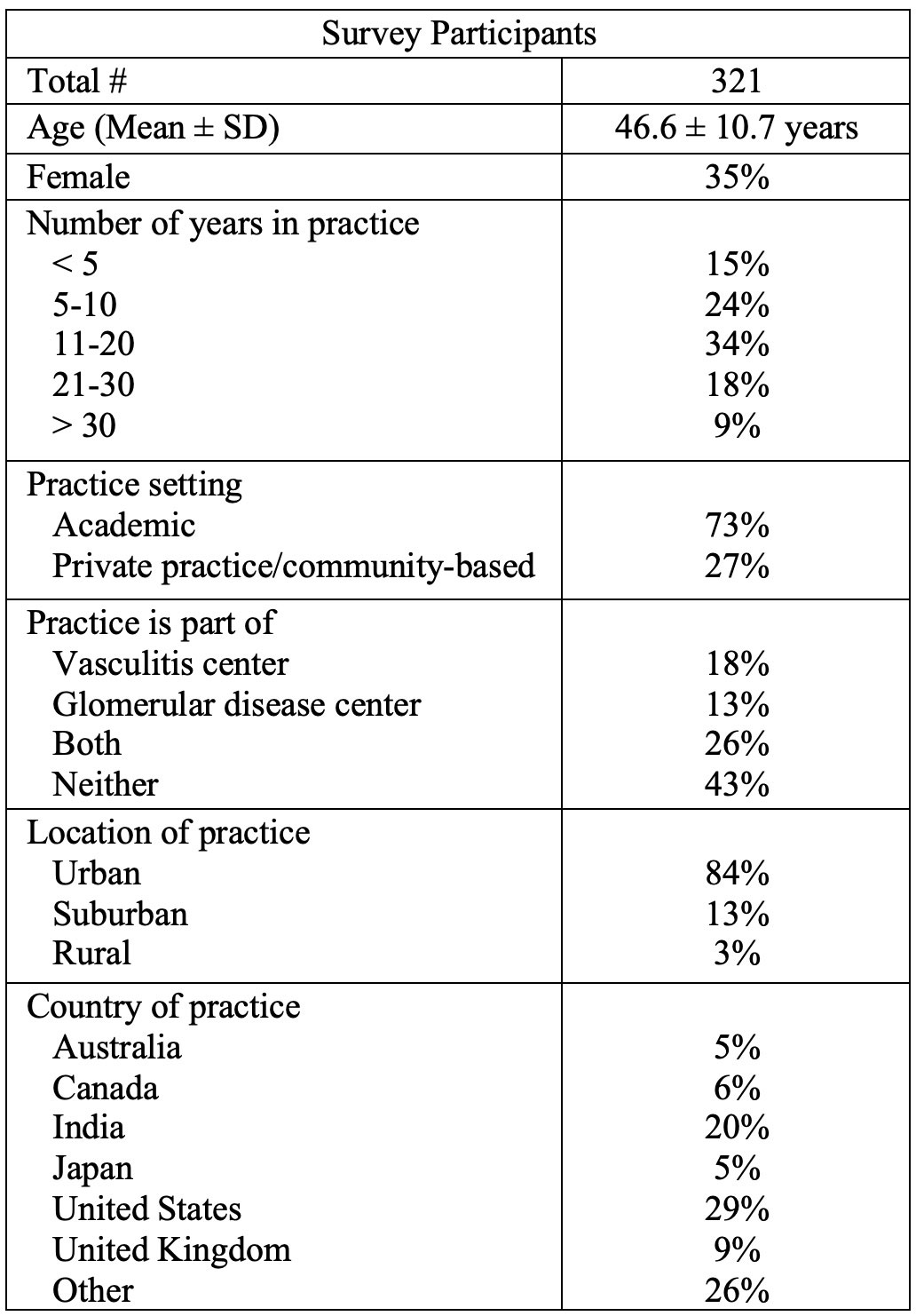
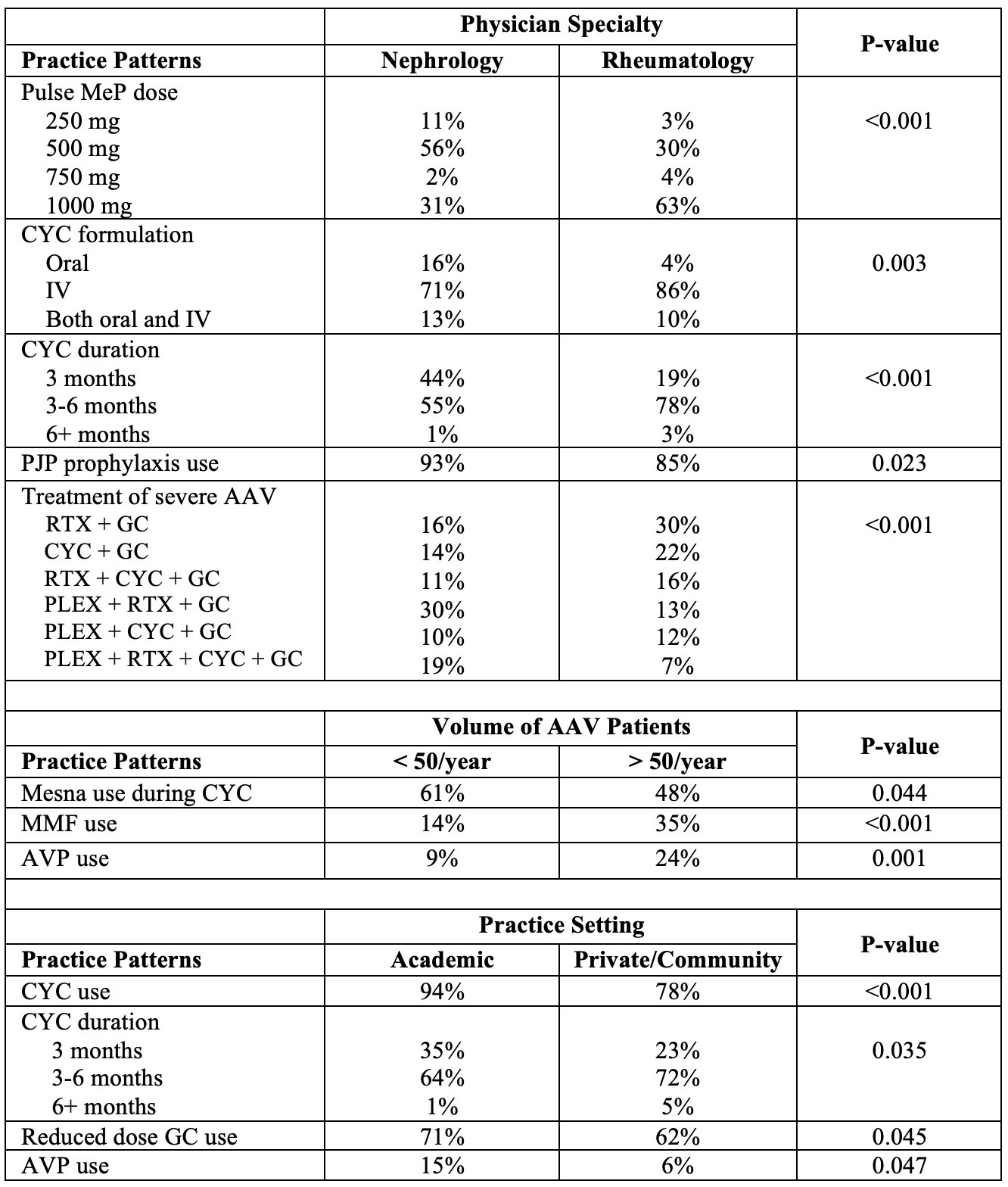
Results: There were 321 total survey participants, of which 53% were nephrologists and 41% were rheumatologists [Table 1]. Of all participants, 29% practiced in the United States, 20% in India, 9% in the United Kingdom, 6% in Canada, and the remainder in other countries. Furthermore, 73% of survey responses came from an academic setting, while 27% came from private practice or a community-based setting. Between the nephrologists and rheumatologists who participated in the survey, there were significant differences observed for the proportions of patients seen with PR3+ ANCA (p < 0.001), MPO+ ANCA (p < 0.001), and ANCA-negative (p = 0.001) disease. Pulse methylprednisolone (MeP) was used by 94%, reduced dose GC by 69%, PLEX by 39%, rituximab (RTX) by 92%, cyclophosphamide (CYC) by 90%, and AVP by 12%. There were significant differences in use of reduced dose GC (p < 0.001, p = 0.001), PLEX (p < 0.001, p = 0.011), RTX brand (p = 0.001, p = 0.010), methotrexate (MTX) [p < 0.001, p < 0.001], and bisphosphonates or denosumab (p < 0.001, p = 0.002) based on physician specialty and AAV patient volume, respectively [Table 2]. Significant differences were also observed in regards to pulse MeP dose (p < 0.001), CYC route and duration (p = 0.003, p < 0.001), use of PJP prophylaxis (p = 0.023) and treatment of severe AAV presentations (p < 0.001) by physician specialty; mesna use during CYC therapy (p = 0.044), mycophenolate mofetil (MMF) use (p < 0.001), and AVP use (p = 0.001) by volume of AAV patients; and CYC use (p < 0.001) and duration (p = 0.035), reduced dose GC use (p = 0.045), and AVP use (p = 0.047) by practice setting [Table 3].
Conclusion: Our survey highlights significant differences in AAV induction therapy practices based on physician specialty, practice setting, and AAV patient volume. Considering reduced dose GC as a recent recommendation, our survey interestingly highlighted that the adoption of reduced dose GC was more common among physicians in nephrology, with greater patient volume, and in an academic setting. Despite this new recommendation, one third of physicians in the survey continue to use standard GC. With the more controversial recommendation of PLEX, we observed a greater proportion of use by physicians in nephrology and with greater patient volume.

To cite this abstract in AMA style:
Xu L, Aqeel F, Tomar O, Li T, Geetha D. Induction Therapy Patterns for Severe ANCA-associated Vasculitis Differ Based on Physician Specialty, Expertise, and Practice Setting: An International Survey [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/induction-therapy-patterns-for-severe-anca-associated-vasculitis-differ-based-on-physician-specialty-expertise-and-practice-setting-an-international-survey/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/induction-therapy-patterns-for-severe-anca-associated-vasculitis-differ-based-on-physician-specialty-expertise-and-practice-setting-an-international-survey/