Session Information
Date: Tuesday, November 10, 2015
Title: Rheumatoid Arthritis - Clinical Aspects IV: Biomarkers, Disease Progression and Treatment Response
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Higher levels of circulating adiponectin
have been linked to radiographic progression in RA in observational studies,
but never studied in the context of early RA with multiple treatment strategies.
Methods: We studied enrollees in the Treatment of Early
Aggressive RA (TEAR) Trial. Participants had early, active RA, were seropositive,
or had ≥2 baseline erosions. All received methotrexate and either etanercept
[immediately (IE) or as step-up therapy (SE)] or sulfasalazine +
hydroxychloroquine (i.e triple therapy) [immediately (IT) or as step-up therapy
(ST)]. Radiographs (baseline, and wks 48 and 102) were obtained and Sharp-van
der Heijde scores (SHS) calculated blind to sequence. Available stored
baseline and 48wks serum samples from patients with complete radiographic data
were assayed for total adiponectin using a bead-based Luminex assay (R&D Systems).
Assays were optimized, run in duplicate, and blocking for RF was used. Multivariable
(MV) generalized linear modeling was used to model SHS change according to
baseline and change in adiponectin level, adjusting for relevant confounders.
Results: A total of 288 patients were studied. Baseline
characteristics (mean age=51 yrs; 70% female; 74% non-Hispanic White; 91%
seropositive for RF or anti-CCP; median RA duration=1.2 months; mean
DAS28-ESR=5.8) were similar to those of the entire trial cohort. Baseline
radiographic damage was observed in 86%, with a median SHS of 2.5 units.
Median baseline adiponectin was 8.6 mg/L, and higher levels at week 48 were
observed in 46% of patients. Factors significantly associated with increasing
adiponectin included female sex, lower baseline adiponectin, EULAR good
response at 48 weeks, and randomization to the IT group. Radiographic
progression (≥2 unit increase in SHS) was observed in 10% at 48 wks. MV
factors significantly associated included higher age, higher baseline ESR and
swollen joint count (SJC), longer RA duration, and increase in adiponectin. Seropositivity,
baseline erosions, baseline adiponectin, BMI, and changes in DAS, ESR, or SJC
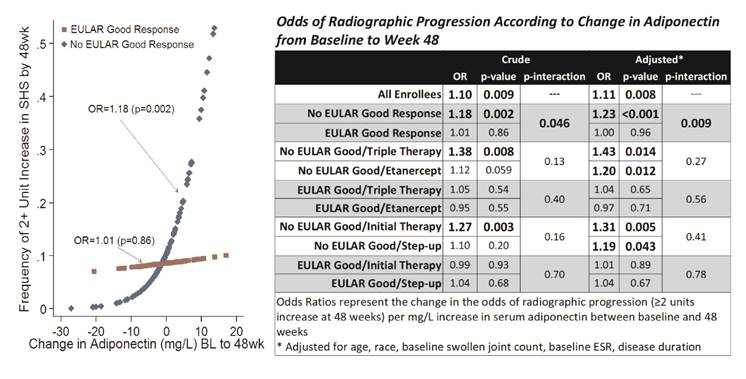
were not associated. For adiponectin, each mg/L increase from baseline to
48wks was associated with a 10% higher odds of radiographic progression (OR=1.10;
p=0.009), an effect not altered with adjustment (Figure). Interestingly, this
effect was observed only in patients without a 48wk EULAR good response
(Figure), and was seen regardless of randomized treatment allocation (Figure). Similar
effects were observed for predicting radiographic progression at 102wks.
Conclusion: Rising adiponectin in the setting of
treatment non-response was a potent factor associated with radiographic
progression among RA patients at highest risk for joint damage in the early
phases of disease. Additional mechanistic studies are needed to define the
physiologic basis for these findings.
To cite this abstract in AMA style:
Giles JT, Bridges SL Jr., O'Dell JR, Cofield S, Howard G, Curtis JR, Moreland LW. Increasing Circulating Adiponectin after DMARD Initiation Is Associated with Radiographic Progression in Early Aggressive RA, Regardless of Treatment Strategy [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/increasing-circulating-adiponectin-after-dmard-initiation-is-associated-with-radiographic-progression-in-early-aggressive-ra-regardless-of-treatment-strategy/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/increasing-circulating-adiponectin-after-dmard-initiation-is-associated-with-radiographic-progression-in-early-aggressive-ra-regardless-of-treatment-strategy/