Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: African Americans have higher rates of SLE and SLE nephritis compared to Caucasians. These epidemiologic associations come mainly from cohort studies that collect standardized information on SLE-related conditions but may not take advantage of the longitudinal data on comorbidities in the electronic health record (EHR). We assessed differences in comorbidities in African Americans vs. Caucasians with SLE using an EHR-based phenome-wide association study (PheWAS). Similar to genome-wide association studies, a PheWAS compares two groups using ICD-9 codes in place of single nucleotide polymorphisms.
Methods: We used our validated algorithm of ≥ 4 counts of the SLE ICD-9 code (710.0) and ANA positive > 1:160 while excluding dermatomyositis and systemic sclerosis ICD-9 codes to identify SLE cases in a de-identified EHR called the Synthetic Derivative (SD). The SD contains over 2.5 million subjects with clinical data collected longitudinally over several decades. Our algorithm has an internally validated positive predictive value of 94% and a sensitivity of 86%. PheWAS was performed in African Americans vs. Caucasians adjusting for age and sex in logistic regression models and correcting for multiple testing using Bonferroni. PheWAS excludes subjects that have a one time count for an ICD-9 code to minimize the effect of coding errors.
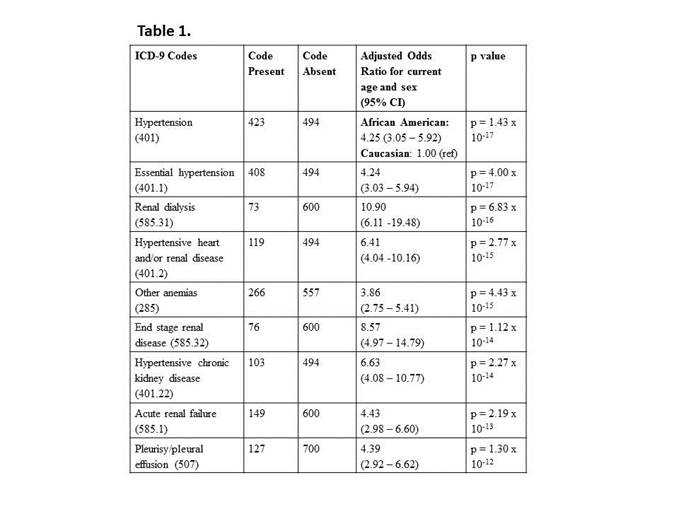
Results: We identified 270 African Americans and 715 Caucasians with SLE. African Americans and Caucasians were predominantly female (89% vs. 90%, p = 0.83) with African Americans having a significantly younger current mean age (44 ± 17 vs. 53 ± 17, p < 0.001) and age at first SLE ICD-9 code (35 ± 16 vs. 43 ± 17, p < 0.001) with similar mean years of follow-up in the EHR (9 ± 5 vs. 10 ± 5, p = 0.10). Adjusting for sex and current age, compared to Caucasians, African Americans had 48 ICD-9 based phenotypes that met the Bonferroni threshold for significance (p < 1.30 x 10–4) including mostly renal and cardiac codes. The most significant codes were hypertension odds ratio (OR) = 4.25 (95% CI 3.05 – 5.92), p = 1.43 x 10-17, renal dialysis OR = 10.90 (95% CI 6.11 – 19.48), p = 6.83 x 10-16, and hypertensive heart and/or renal disease OR = 6.41 (95% CI 4.04 – 10.16), p = 2.77 x 10-15 (Table 1). Compared to Caucasians, African Americans were more likely to have codes related to SLE ACR criteria including pleurisy/pleural effusion, nephritis, pericarditis, pancytopenia, and joint effusions (all p < 0.05).
Conclusion: Using a large EHR, we found that African Americans had more codes related to ACR SLE criteria including renal disease as well as hypertension. While in the general population African Americans are twice as likely to have hypertension compared to Caucasians, our data show an even more pronounced effect in African Americans vs. Caucasians with SLE. Additional studies are needed to determine the mechanisms for this racial disparity.
To cite this abstract in AMA style:
Barnado A, Carroll R, Casey C, Denny JC, Crofford LJ. Increased Hypertension and Renal Disease in African Americans Compared to Caucasians with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/increased-hypertension-and-renal-disease-in-african-americans-compared-to-caucasians-with-systemic-lupus-erythematosus/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/increased-hypertension-and-renal-disease-in-african-americans-compared-to-caucasians-with-systemic-lupus-erythematosus/