Session Information
Session Type: Abstract Submissions (ACR)
TITLE: “Incidence of knee, hip, and hand clinical osteoarthritis: a population-based cohort study.”
AUTHORS: Daniel Prieto-Alhambra*, Aina Pag�s-Castellˆ, M Kassim Javaid, Andrew Judge, Cyrus Cooper, Nigel K Arden, and Adolfo Diez-Perez
* Presenting author
2,496 / MAX 2,750 CHARACTERS
Background/Purpose:
Data on age-specific effects of gender, obesity and previous osteoarthritis (OA) on incident OA at other joints are scarce. We aimed to calculate age and gender-specific incidence of joint-specific clinical OA. Secondly, we studied the age-dependent effect of gender, and the excess risk related to obesity and previous OA on newly diagnosed OA at the knee, hip and hand.
Methods:
We screened computerized medical records in the SIDIAP Database (www.sidiap.org) to identify those aged 40 years or older with an incident diagnosis of OA of the knee, hip and hand using ICD-10 codes in the period 2006-2010. SIDIAP contains the anonymised medical records of >3,100 GPs in Catalonia (North-East Spain) with information on an 80% of the total population. Age and gender-specific incidence rates (IR), Female:Male Rate Ratios (RR), and 95%Confidence Intervals (99%CI) were calculated assuming a Poisson distribution. Cox regression was used to compute adjusted (for age, gender, and body mass index(BMI)) hazard ratios (HR) for a new diagnosis of OA according to BMI (WHO categories) and to prevalent joint-specific OA status.
Results:
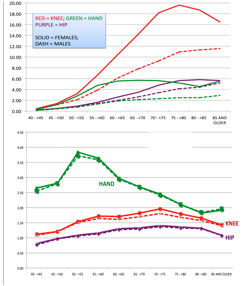
We identified 26,381, 12,567 and 10,092 incident cases of knee, hip and hand OA respectively. Age-specific IRs for knee, hip, and hand OA are shown [Figure]. Female:Male RRs peaked at age 70-75 years for hip and knee, and at the age of 50-55 years for hand OA [Figure]. Adjusted HRs for BMI categories were highest for knee OA (overweight = HR 2.00 (99%CI 1.94-2.06), obesity 1 = HR 3.19 (3.09-2.30), obesity 2 = HR 4.72 (4.56-4.89)), followed by hip OA (HR 1.46 (1.39-1.52); 1.75 (1.66-1.83); 1.93 (1.82-2.05)), and lower for hand OA (HR 1.22 (1.17-1.27), 1.30 (1.25-1.36) and 1.31 (1.24-1.38)).
Adjusted HR for prevalent knee OA on hip OA was 1.35 (1.28-1.43); HR for previous hip OA on incident knee OA was 1.15 (1.08-1.23). Hand OA predicted both knee and hip OA (HR 1.20 (1.14-1.26) and 1.23 (1.13-1.34) respectively).
Conclusion :
Age, gender, BMI and history of OA affecting other joints are related differently to incident knee, hip and hand OA: both the effect of age and gender are greatest in the elderly for knee and hip OA, but around menopause for hand OA. The effect of overweight and obesity is strongest on knee OA, and weakest but significant on hand OA. Finally, a history of knee or hip OA predict incidence of each other, and previous hand OA is related to increased risk of knee and hip OA, all independently of age, gender and BMI.
Figure. Age and gender-specific IR (/1,000 person-years) of knee, hip and hand OA [Top], and unadjusted (solid) and adjusted (dash) Female:Male RR [Below].
Disclosure:
D. Prieto-Alhambra,
None;
A. Pagès-Castellà,
None;
M. K. Javaid,
None;
A. Judge,
None;
C. Cooper,
Amgen, ABBH, Novartis, Pfizer, Merck Sharp and Dohme, Eli Lilly, Servier,
5;
N. K. Arden,
None;
A. Díez-Pérez,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incidence-of-knee-hip-and-hand-clinical-osteoarthritis-a-population-based-cohort-study/