Session Information
Date: Monday, October 27, 2025
Title: (1147–1190) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial pneumonia with autoimmune features (IPAF) is a type of interstitial lung disease (ILD) with features of autoimmunity, yet patients do not fulfill criteria for any defined systemic autoimmune rheumatic diseases (SARDs)(1). Classification of IPAF requires the presence of interstitial pneumonia and presence of features from at least two of three domains: serological (specific autoantibodies), clinical (signs and symptoms which may be seen in SARDs) and morphological (imaging or biopsy features within the thorax suggestive of ongoing inflammation) (1). While previously thought to be rare (2), a recent study revealed that 31% of ILD patients undergoing lung transplant are classified as IPAF (3). Studies of IPAF are limited by its lack of diagnostic criteria and propensity to be studied only at large tertiary referral centers. There are therefore no population-based studies of IPAF, which limits our understanding of its incidence and prevalence.
Methods: We conducted a population-based study to establish the incidence and prevalence of IPAF in a geographically defined area between 2010-2019. Prevalence was calculated on January 1st, 2020. We screened all patients with 2+ ILD codes as well as abnormal autoimmune serologies and/or 2+ codes for Raynaud’s syndrome. We excluded all patients with 2+ SARD codes. We performed manual chart review and radiographic review to validate IPAF classification criteria (1) and presence of ILD. We collected data on the presence and specific features of each of the three domains included in IPAF classification: serological, clinical, and morphological (1). Date of IPAF incidence was considered the date of first ILD diagnosis. Descriptive statistics were utilized to describe the baseline characteristics of the cohort. Age- and sex-specific incidence rates were calculated using the number of incident cases as the numerator and census estimates as the denominator. Overall incidence rates were age- and/or sex-adjusted to the 2020 white population of the USA. Confidence intervals for incidence rates were obtained by assuming that the number of incident cases followed a Poisson distribution.
Results: After manual review, a total of 33 patients had confirmed incident IPAF. Table 1 describes the baseline features of those with incident IPAF. The incidence of IPAF was greater in women than in men and increased with age (Table 2). Overall, the annual sex-and age-adjusted IPAF incidence was 3.2 per 100,000 persons. On January 1, 2020, there were 30 patients with prevalent IPAF corresponding to a sex- and age-adjusted IPAF prevalence rate of 26 per 100,000 persons.
Conclusion: To our knowledge, this is the first population-based cohort study of IPAF incidence and prevalence. IPAF is a rare disease, with low prevalence and low incidence rates which are higher in women than men and increase with age. Future studies will expand on the cohort and will include study of phenotypes among IPAF patients and relationship with clinical outcomes.
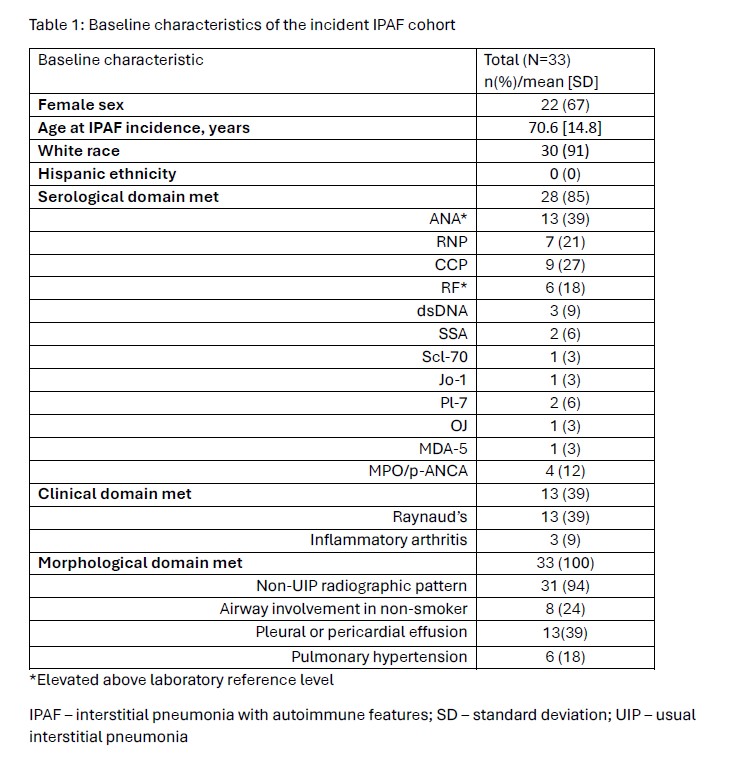 Table 1: Baseline characteristics of the incident IPAF cohort
Table 1: Baseline characteristics of the incident IPAF cohort
*Elevated above laboratory reference level
IPAF – interstitial pneumonia with autoimmune features; SD – standard deviation; UIP – usual interstitial pneumonia
.jpg) Table 2: Incidence rates for IPAF
Table 2: Incidence rates for IPAF
*Age- and sex- adjusted to the United States White population (USW2020)
IPAF – interstitial pneumonia with autoimmune features
.jpg) References
References
To cite this abstract in AMA style:
Joerns e, Achenbach S, Crowson C, carmona e, Vassallo R, Joerns J, Kronzer V, Davis J, myasoedova E. Incidence and Prevalence of Interstitial Pneumonia with Autoimmune Features in a Population-Based Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/incidence-and-prevalence-of-interstitial-pneumonia-with-autoimmune-features-in-a-population-based-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incidence-and-prevalence-of-interstitial-pneumonia-with-autoimmune-features-in-a-population-based-cohort/