Session Information
Date: Monday, November 9, 2020
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: In radiographic axial spondyloarthritis (r-axSpA), spinal damage manifests as syndesmophytes and facet joint ankylosis (FJA). Whether there is an order in which lesion develops first is unknown.
Methods: Data were used from the Sensitive Imaging in Ankylosing Spondylitis (SIAS) cohort from Leiden and Herne. Inclusion criteria were: clinical r-axSpA diagnosis, ≥1 inflammatory lesion on spinal Magnetic Resonance Imaging (MRI), ≥1 and ≤18 syndesmophytes on conventional radiography of lateral cervical and lumbar spine, and fulfillment of the modified New York criteria. Patients underwent low-dose Computed Tomography (ldCT) at baseline and two-years. LdCT images were scored independently by two trained readers. Vertebrae were scored according to the Computed Tomography Syndesmophyte Score (CTSS) for presence and size of syndesmophytes; facet joints were scored as not-ankylosed and ankylosed. Analyses were performed on the vertebral unit (VU) level and using individual-reader data (Figure). Two hypotheses were tested: 1) presence of bridging syndesmophyte(s) is associated with FJA on the same VU two years later, and 2) presence of FJA is associated with syndesmophyte(s) on the same VU two years later. Generalized Estimating Equations (GEE) models were used to take into account the correlations between VUs from the same patient and adjusting for reader to account for individual reader scores. Two models were tested per hypothesis using different outcomes. Model 1 uses the presence of syndesmophytes or FJA as outcome adjusting for the outcome at baseline. Model 2 uses development of new syndesmophytes or FJA at two years plus an increase in the number of syndesmophytes or FJA.
Results: In total, 50 patients were included (mean age 49, 84% male, 82% HLA-B27+). At baseline, there was a higher percentage of bridging syndesmophytes (range: 10-60%) than FJA (range: 8-36%) considering all VUs and both readers (Figure). In both models, presence of bridging syndesmophytes was associated with development of FJA two years later (OR (95%CI) Model 1: 3.35 (2.18-5.14); Model 2: 2.23 (1.19-4.16)) while presence of FJA at baseline did not have a statistically significant association with development of syndesmophytes two years later (Table).
Conclusion: The data showed a higher occurrence of bridging syndesmophytes than FJA at baseline and showed significantly increased odds to develop FJA when bridging syndesmophyte(s) are present on the same VU two years prior. This mechanism did not hold true for the other direction. These results cautiously imply that in our study population with advanced r-axSpA bridging syndesmophytes precede FJA, rather than FJA preceding syndesmophytes.
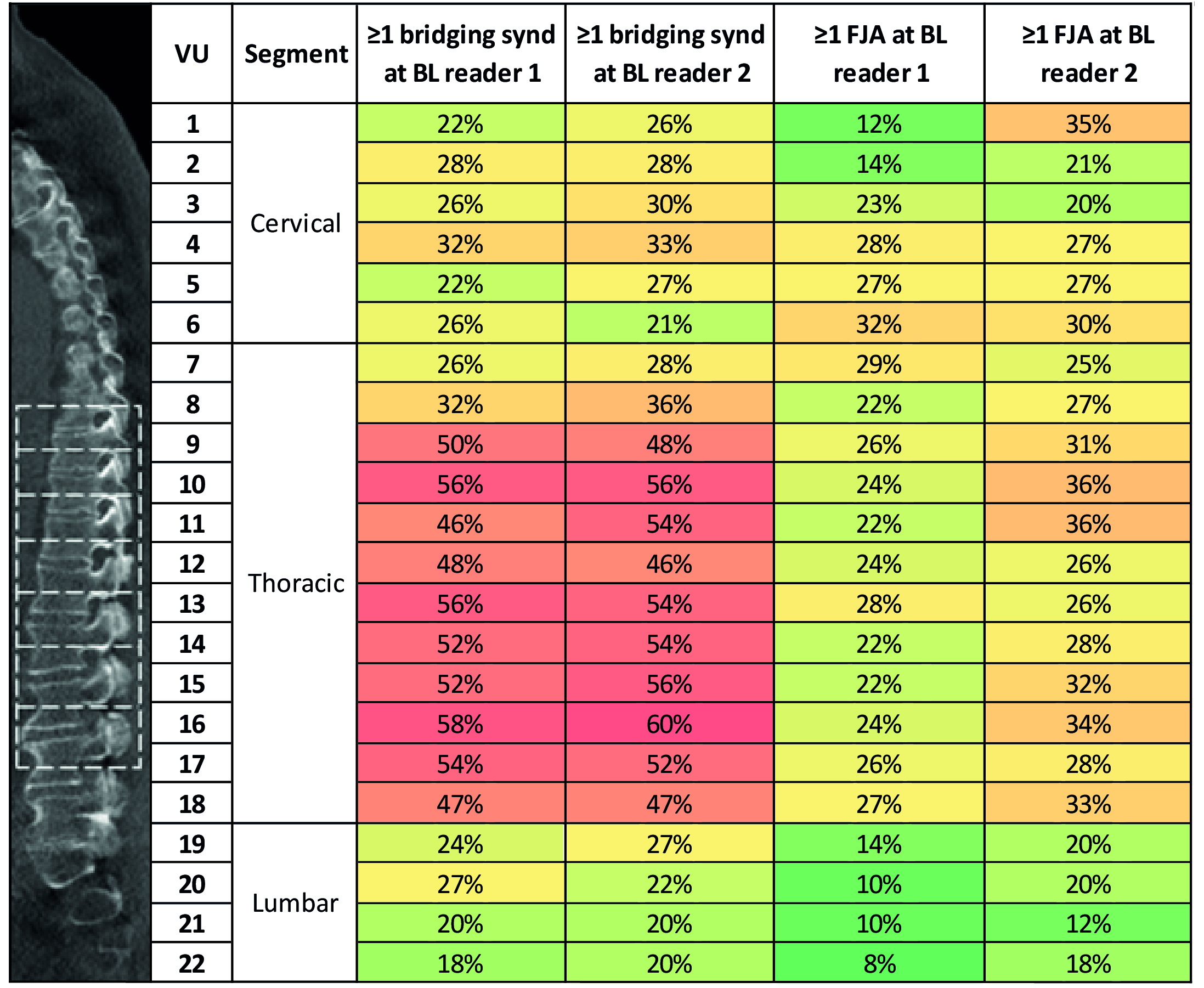 Figure: Percentage of occurrence of syndesmophytes and facet joint ankylosis per vertebral unit and per reader at baseline. Figure displaying percentages of patients with a bridging syndesmophyte and with facet joint ankylosis at baseline, per reader. The image on the left illustrates the vertebral unit level (VU) at which analyses were performed. Seven VUs are illustrated in dashed boxes as example. Synd, syndesmophyte; FJA, facet joint ankylosis; BL, baseline.
Figure: Percentage of occurrence of syndesmophytes and facet joint ankylosis per vertebral unit and per reader at baseline. Figure displaying percentages of patients with a bridging syndesmophyte and with facet joint ankylosis at baseline, per reader. The image on the left illustrates the vertebral unit level (VU) at which analyses were performed. Seven VUs are illustrated in dashed boxes as example. Synd, syndesmophyte; FJA, facet joint ankylosis; BL, baseline.
 Table: Results of the GEE analyses of the two hypotheses Model 1 was adjusted for the outcome at baseline and both models were adjusted for the reader level, not shown in the table. Statistically significant odds ratios are presented in bold. FJA, facet joint ankylosis; BL, baseline; FU, follow-up
Table: Results of the GEE analyses of the two hypotheses Model 1 was adjusted for the outcome at baseline and both models were adjusted for the reader level, not shown in the table. Statistically significant odds ratios are presented in bold. FJA, facet joint ankylosis; BL, baseline; FU, follow-up
To cite this abstract in AMA style:
Stal R, Sepriano A, van Gaalen F, Baraliakos X, van den Berg R, Reijnierse M, Braun J, Landewé R, van der Heijde D. In Radiographic Axial Spondyloarthritis, Bridging Syndesmophytes Increase Risk of Facet Joint Ankylosis Development on the Same Vertebral Level While Facet Joint Ankylosis Does Not Increase Risk of Same Level Syndesmophytes Development [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/in-radiographic-axial-spondyloarthritis-bridging-syndesmophytes-increase-risk-of-facet-joint-ankylosis-development-on-the-same-vertebral-level-while-facet-joint-ankylosis-does-not-increase-risk-of-sa/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/in-radiographic-axial-spondyloarthritis-bridging-syndesmophytes-increase-risk-of-facet-joint-ankylosis-development-on-the-same-vertebral-level-while-facet-joint-ankylosis-does-not-increase-risk-of-sa/