Session Information
Session Type: ACR Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: To improve Pneumococcal Vaccination rates in high risk Rheumatology patients on immunosuppressive therapy.
Methods: The study was a quality improvement project based on the pre-post-intervention design. The phase I of the project targeted all Rheumatoid Arthritis patients on immunosuppressive therapy for pneumovax vaccine (PV) seen in thirteen Rheumatology outpatient clinics (1/2013 to 7/2015). In the Phase II study (1/2015-10/2017) all Rheumatology patients on immunosuppressive medications irrespective of their diagnosis were intervened for pneumovax and prevnar vaccination as per current CDC guidelines. The electronic Best Practice Alert (BPA) for both PVs were developed with backend algorithm based on CDC guidelines. Based on patient eligibility checked electronically, the appropriate PV appeared on electronic medical records at the time of rooming of the eligible patient by the medical assistant. BPA was designed to inform the physician about vaccination status as well as enable physician to easily order PV or document refusal or deferral reasons (Figure 1). Education regarding vaccine guidelines, BPA, vaccination process, and regular feedback of results were important components of the project interventions. The vaccination rates during pre-post intervention phases during each study phase were compared using Chi square test.
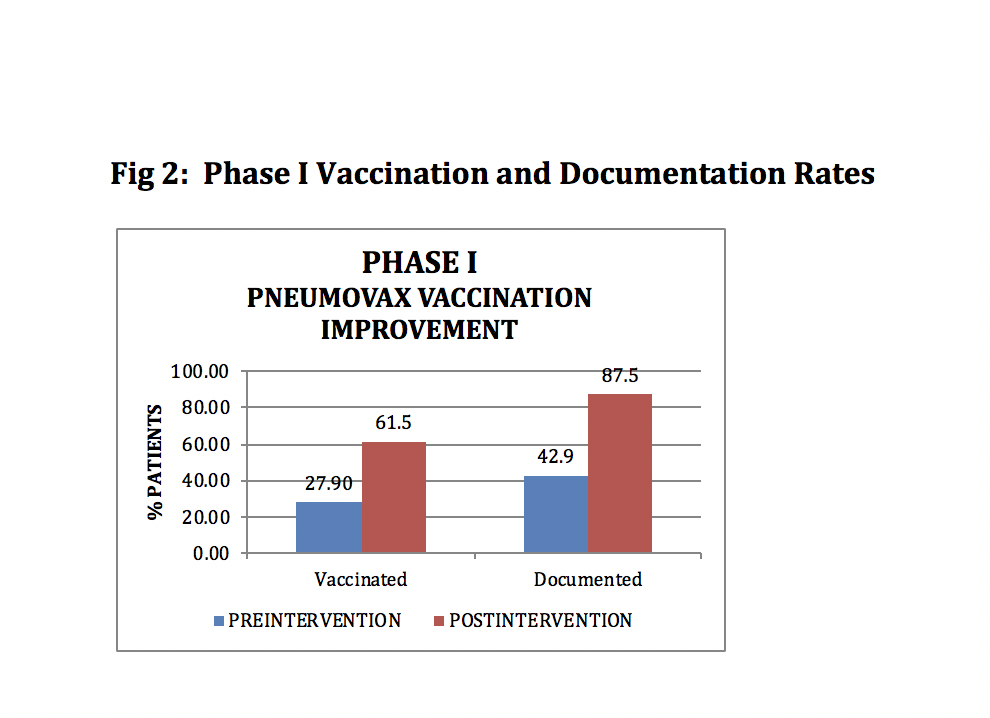
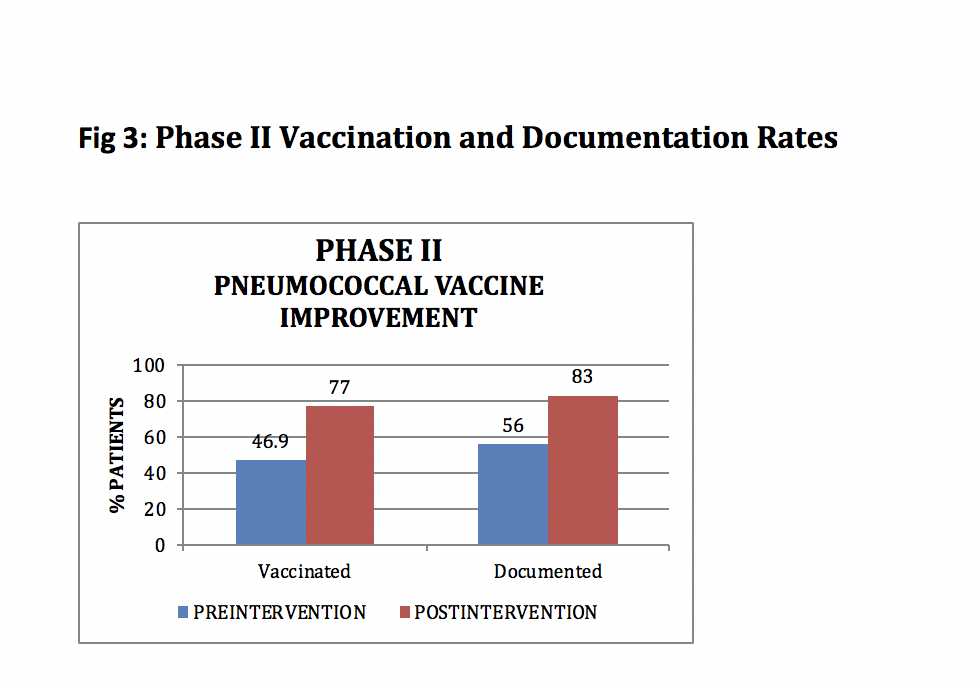
Results: The PV rates reported as patients vaccinated among all eligible patients, improved significantly during both study phases. Phase I demonstrated 61.5% Pneumovax vaccination rate compared to pre-intervention rate of 27.9 % (p< 0.0001) (Figure 2). During Phase II 77% patients had received either pneumovax or prevnar compared to 49.6% patients in pre-intervention period (p< 0.0001) (Figure 3). The documentation rates (vaccine received, ordered, patient refusal and deferral reasons) also increased significantly in both phases. `
Conclusion: Electronic identification of vaccine eligibility and implementation of BPA with capabilities to order and document reasons for non-compliance significantly improved PV rates. The process required minimal modification of clinic work flow, and did not increase physician time. The project was self- sustained during Phase II with initial education and thus has potential for self-sustainability and generalizability.

To cite this abstract in AMA style:
Sheth H, Vera G, Rudge D, Fischer G, Moreland L, Aggarwal R. Improving Pneumococcal Vaccination Rates in High Risk Rheumatology Patients [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/improving-pneumococcal-vaccination-rates-in-high-risk-rheumatology-patients/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-pneumococcal-vaccination-rates-in-high-risk-rheumatology-patients/