Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a systemic small vessel vasculitis associated with significant morbidity and complex care needs across a broad demographic spectrum. While prior studies have demonstrated an increased prevalence of mental health disorders among patients with AAV, the impact of pre-existing psychiatric conditions on disease outcomes remains insufficiently characterized. Given the potential interplay between psychiatric comorbidities and systemic inflammation, further investigation is warranted. This study aims to evaluate the influence of pre-existing psychiatric disorders on clinical outcomes and treatment patterns in adult patients diagnosed with AAV.
Methods: We conducted a retrospective cohort study using the TriNetX network, comparing adult AAV patients with and without pre-existing psychiatric diagnoses (schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, or persistent mood disorder). Propensity score matching was performed for age, sex, race, and smoking status. Five-year incident risk of chronic renal disease, pulmonary disease, infections, venous thromboembolism, glucocorticoid use, and glucocorticoid-associated toxicities were compared using relative risk (RR) with 95% confidence intervals (CI). The ICD-10 and RxNorm codes corresponding to these outcomes, as defined within the TriNetX database, are presented in Table 1.
Results: A total of 1,121 AAV patients with preexisting psychiatric disorders and 17,465 without were included, with 1,116 patients in each cohort after matching (Table 2). Before matching, psychiatric comorbidity was associated with higher risks of acute kidney failure (RR 1.31, 95% CI 1.04–1.64), respiratory failure (1.59, 1.29–1.95), venous thromboembolism (1.37, 1.02–1.86), and infections. After matching, psychiatric comorbidity remained associated with increased risks of pneumonia (1.45, 1.09–1.94), skin infections (1.93, 1.40–2.67), sepsis (1.41, 1.01–1.96), and viral infections (1.55, 1.13–2.13). In unmatched analyses, patients with psychiatric disorders were more likely to be prescribed glucocorticoids (1.13, 1.09–1.18) and less likely to receive glucocorticoid-sparing immunosuppressants (0.81, 0.71–0.92); the latter association persisted after matching (Figure 1).
Conclusion: In AAV, pre-existing psychiatric disorders are associated with increased infectious complications and decreased prescription of glucocorticoid-sparing therapies. Future research should investigate potential co-inflammatory interactions between psychiatric disorders and AAV, and socioenvironmental factors influencing medication adherence and access to care.
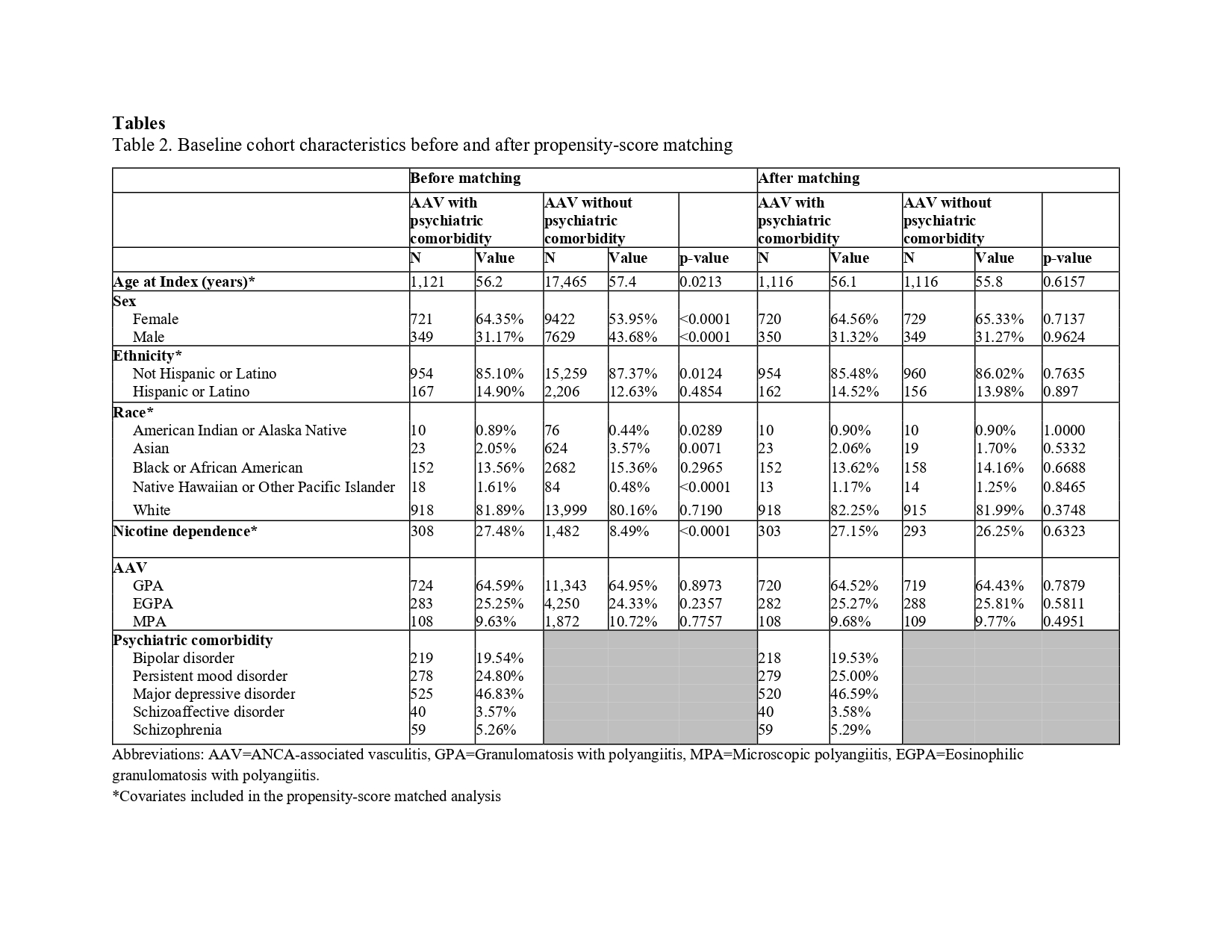
.jpg) Abbreviations: AAV=ANCA-associated vasculitis, GPA=Granulomatosis with polyangiitis, MPA=Microscopic polyangiitis, EGPA=Eosinophilic granulomatosis with polyangiitis.
Abbreviations: AAV=ANCA-associated vasculitis, GPA=Granulomatosis with polyangiitis, MPA=Microscopic polyangiitis, EGPA=Eosinophilic granulomatosis with polyangiitis.
*Covariates included in the propensity-score matched analysis
.jpg) Relative risk of 5-year incident outcomes in adult ANCA-associated vasculitis (AAV) patients with a pre-existing psychiatric comorbidity. The reference group for both plots is the cohort of adult patients with AAV and no documented psychiatric disorder (schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, or persistent mood disorder) at any time point. Plot A shows the unadjusted analyses and plot B displays the adjusted analyses after propensity-score matching for age at AAV diagnosis, sex, race, and nicotine dependence in a 1:1 ratio between the cohort of interest and the reference cohort. The dashed gray vertical line in both plots represents no difference in relative risk between the cohorts. Plots highlighted in red indicate a statistically significant difference between cohorts.
Relative risk of 5-year incident outcomes in adult ANCA-associated vasculitis (AAV) patients with a pre-existing psychiatric comorbidity. The reference group for both plots is the cohort of adult patients with AAV and no documented psychiatric disorder (schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, or persistent mood disorder) at any time point. Plot A shows the unadjusted analyses and plot B displays the adjusted analyses after propensity-score matching for age at AAV diagnosis, sex, race, and nicotine dependence in a 1:1 ratio between the cohort of interest and the reference cohort. The dashed gray vertical line in both plots represents no difference in relative risk between the cohorts. Plots highlighted in red indicate a statistically significant difference between cohorts.
To cite this abstract in AMA style:
Patel S, Denvir B, Kaltchenko M, Bao A, Simha V, Cammarata M, Kang J. Impact of psychiatric comorbidity on disease outcomes in ANCA-associated vasculitis: A multi-center retrospective cohort study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/impact-of-psychiatric-comorbidity-on-disease-outcomes-in-anca-associated-vasculitis-a-multi-center-retrospective-cohort-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impact-of-psychiatric-comorbidity-on-disease-outcomes-in-anca-associated-vasculitis-a-multi-center-retrospective-cohort-study/