Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Giant cell arteritis (GCA) affects medium and large arteries. Although temporal artery biopsy (TAB) remains the gold standard for patients with cranial GCA, patients with large-vessel GCA may not have confirmatory histologic findings on TAB. The most recent guidelines recommend vascular imaging in the management of GCA to better assess large vessels. In this study, we examine the clinical characteristics of patients with GCA, how additional imaging is currently utilized in the diagnosis of GCA, and whether inter-disciplinary teams are associated with differences in management.
Methods: Subjects through the Dallas VAMC database from 2010-2021 were identified via ICD-9/10 codes for GCA, polymyalgia rheumatica, and through a TAB list from the pathology lab. Those without sufficient data to assess for ACR 1990 classification criteria for GCA were excluded. Fisher’s exact test was used to compare categorical variables among groups. Kruskal-Wallis test was used to compare continuous variables.
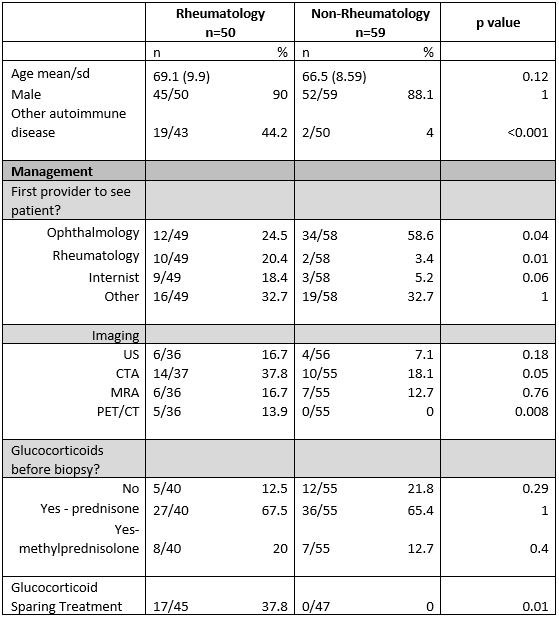
Results: 209 patients were identified. 46 patients were excluded due to lack of sufficient data for ACR classification. 9.2% were female with an average age of 68.4. Ophthalmology was the first encounter provider in 46% of cases. Only 6% of patients had any documentation of vascular assessment (i.e., evaluation of pulses, blood pressure in both arms, listening for bruits). Of the remaining 163 patients, 35 had a final diagnosis of GCA and 15 of these had a positive TAB (Table 1). The most common presenting symptoms were visual symptoms (75.1%) and headache (67.2%), with significant differences for headache seen among TAB-positive GCA, TAB-negative GCA, and non-GCA groups (p = 0.01). TAB-negative GCA were more likely to have scalp tenderness when compared to GCA TAB-positive and non-GCA (p = 0.03). A diagnosis of GCA was more likely to be associated with other co-existing autoimmune (AI) disease, glucocorticoid-sparing immunosuppressive treatment, and having a rheumatology provider (p < 0.001). Those with a rheumatology provider were more likely to have co-existing AI disease (< 0.001), to have advanced imaging (Figure 1) such as CTA (p = 0.05) and PET/CT (p = 0.008), and to have glucocorticoid-sparing immunosuppressive treatment (p = 0.02) (Table 2).
Conclusion: GCA presentation is heterogenous and diagnosis is challenging. Scalp tenderness was more likely associated with TAB-negative GCA. Vascular assessments and adjunct diagnostic imaging modalities are infrequently utilized. Rheumatologists are more likely to diagnose and manage patients with a coexistent AI disease, to employ more advanced imaging, and to prescribe glucocorticoid-sparing treatments. Co-management among specialties may optimize management.


To cite this abstract in AMA style:
Agarwal A, Weisberg R, Mathew J, Reimold A, Shwin K. Imaging Use and Medication Management in Giant Cell Arteritis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/imaging-use-and-medication-management-in-giant-cell-arteritis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/imaging-use-and-medication-management-in-giant-cell-arteritis/