Session Information
Date: Sunday, November 12, 2023
Title: (0691–0721) Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Immunoglobulin-A (IgA) Vasculitis (IgAV) is a small-vessel vasculitis that is primarily diagnosed based on the European League Against Rheumatism (EULAR) criteria. There is limited knowledge about the IgAV phenotype in a racially and ethnically diverse population. We aimed to describe the clinicopathologic characteristics of IgAV in our adult skin of color (SOC) patients.
Methods: We retrospectively reviewed adult patients ( >18 years) from the dermatopathology database with leukocytoclastic vasculitis (LCV) at Montefiore Medical Center between January 2012–December 2022 (Figure 1). We collected demographic, clinical, laboratory, and histopathological data from the electronic medical record to identify individuals with SOC who met EULAR criteria. We defined SOC as any non-White race/ethnicity. Descriptive statistics and Fisher’s exact test were used to analyze the SOC cohort.
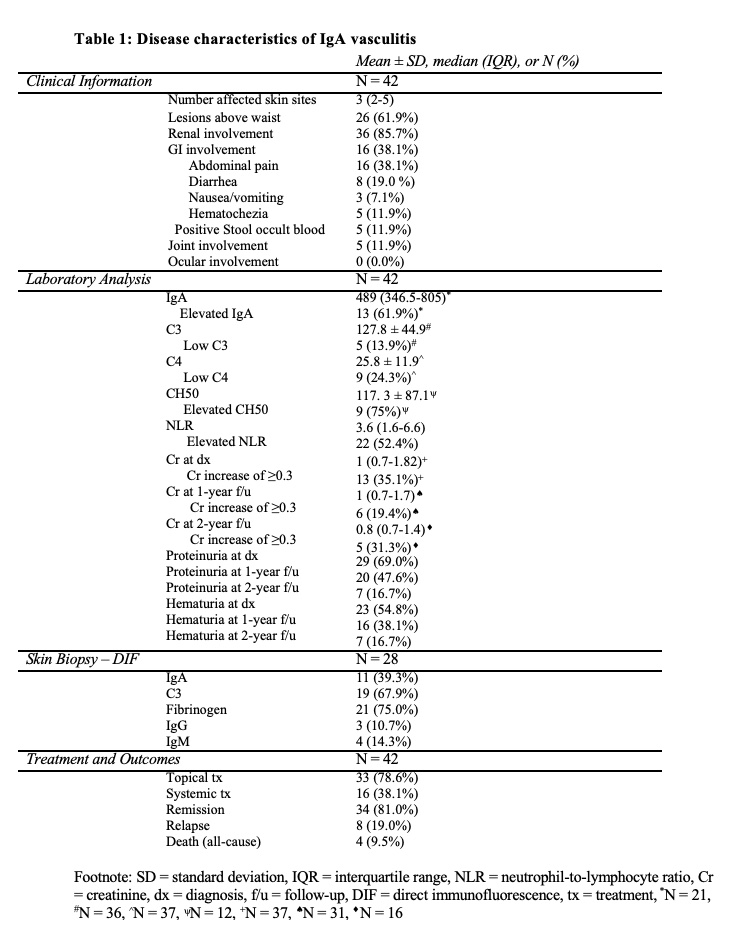
Results: We identified 65 patients with LCV, 52 patients met EULAR criteria for IgAV, of which 42 (81%) were SOC. In our SOC cohort of 42 patients, 32 (76%) identified themselves as Spanish/Hispanic/Latino, 7 (17%) identified themselves as Black, and 3 (7%) identified themselves as Asian. The mean (±SD) age was 56 (±16) years and 29 (69%) were females. The median (IQR) number of affected body sites was 3 (2-5). Renal involvement was present in 36 (86%) patients (Table 1). Gastrointestinal (GI) involvement was present in 16 (38%) and joint involvement was present in 5 (12%). Elevated neutrophil/lymphocyte ratio (NLR) was present in 22 (52%). Elevated serum IgA levels were present in 13 (62%) of the 21 patients with measured serum IgA. Skin biopsy direct immunofluorescence (DIF) was performed in 28 (67%) patients and showed IgA and C3 in 11 (39%) and 19 (64%), respectively. Remission was achieved in 34 (81%) patients and 8 (19%) experienced relapse.
We further analyzed the 28 patients who had skin biopsy with DIF and compared those with and without IgA deposition (Figure 1). The IgA+ group had significantly lower prevalence of renal involvement (p=0.0161), higher prevalence of GI involvement (p=0.0204), high NLR (p=0.0238), and C3 deposition on DIF (p=0.0039), and greater number of affected body sites (p=0.0206). Lesions above waistline and elevated serum IgA were not associated with systemic symptoms, including renal involvement, or positive DIF. Elevated NLR was associated with IgA deposition (p=0.0209).
Conclusion: In contrast to previous studies, the majority of our adult SOC patients had renal or GI involvement with IgA+ DIF being associated with lower prevalence of renal involvement. Additionally, our SOC patients with IgA+ DIF had more widely distributed lesions. Cutaneous involvement above the waist was not associated with renal complications. Prior studies showing the predictive value of skin biopsy and lesion location in predominantly White populations may not apply to SOC patients.

To cite this abstract in AMA style:
Toker M, Khanna U, Nazarian R, Mehta A, Ayesha B, Kumthekar A, Wu B. IgA Vasculitis in a Diverse Adult Patient Population [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/iga-vasculitis-in-a-diverse-adult-patient-population/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/iga-vasculitis-in-a-diverse-adult-patient-population/