Session Information
Date: Tuesday, October 23, 2018
Title: Systemic Lupus Erythematosus – Clinical Poster III: Treatment
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Systemic Lupus Erythematosus (SLE) is a multisystem autoimmune disease with complex genetic background. Recently, subphenotype in SLE has influenced dialogue on discussing the genetic background, disease course, outcomes and treatment. The objective of this study is to identify phenotype clusters within a SLE cohort patients, and compare the genetic risk score (GRS), clinical manifestations and mortality between clusters.
Methods: This is a single center, descriptive study of from Hanyang BAE lupus Cohort. Patients whose disease duration is less than 5 years were excluded to minimize potential confounding effects of disease duration. Mortality data were derived in connection with data from the Korean National Statistics Office. Patients were grouped into 3 clusters based on SLICC Damage Index (SDI) using K-mean cluster analysis. Clinical characteristics were compared using ANOVA and Tukey’s test.
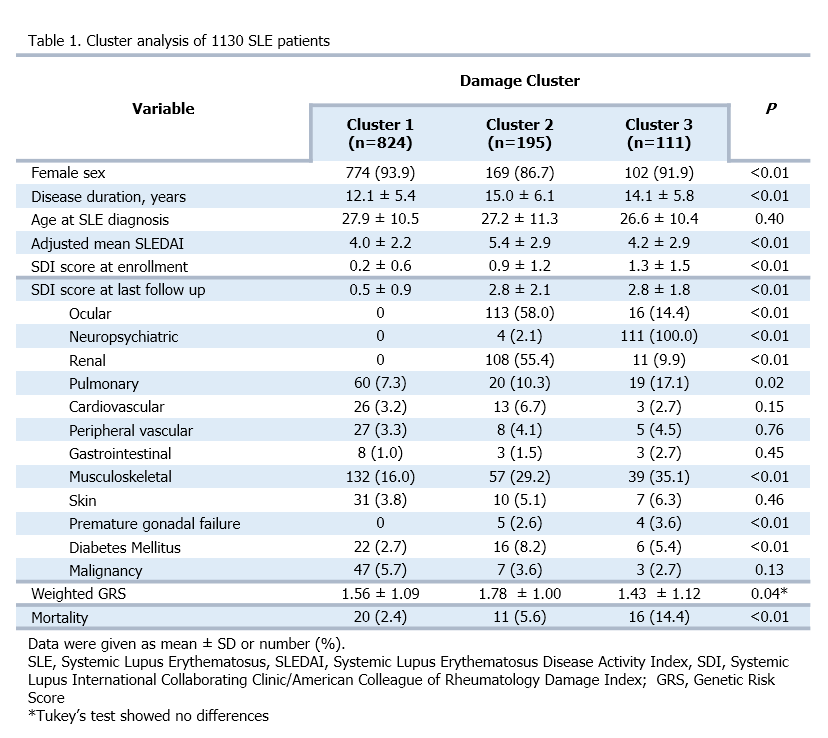
Results: In 1130 analyzed patients, musculoskeletal damage was the most prevalent (20.2%), followed by ocular (11.4%), renal (10.5%) and neuropsychiatric damage (10.2%). Three separate damage clusters were identified, each with significantly different damage manifestations. Cluster 1 (n=824) showed the least damage profile. Cluster 2 (n=195) was represented by the predominance of renal damage (55.4%), with prevalent ocular (58.0%), musculoskeletal (29.2%) damage and diabetes mellitus (8.2%). Cluster 3 (n=111) was characterized by neuropsychiatric damage (100%) with musculoskeletal (35.1%) and pulmonary damage (17.1%). Age of onset of SLE and autoantibody positivity were similar among clusters. Cluster 2, represented by prevalent renal and glucocorticoid associated damages, showed higher adjusted mean SLEDAI score (AMS) (Mean ± SD, 6.7 ± 4.8) than other two clusters. Cluster 3 distinguished by neuropsychiatric damage showed the highest mortality among three clusters. However, GRS showed no difference between 3 clusters after Tukey’s test.
Conclusion: We identified different patterns of damage manifestations in a large cohort of SLE patients. Renal and neuropsychiatric damage were the two distinct domain of damage that classified patients into 3 clinically meaningful clusters. Patients in cluster 2 (prevalent renal and glucocorticoid associated damage) had the highest AMS. The highest mortality was recognized in cluster with prevalent neuropsychiatric damage. However, GRS showed no difference between clusters Further studies assessing comprehensive subphenotypes are needed.
To cite this abstract in AMA style:
Ahn GY, Lee J, Ha E, Kim K, Kim H, Kim JS, Nam B, Kang J, Kwon HH, Bang SY, Lee HS, Bae SC. Identifying Phenotype Clusters in Systemic Lupus Erythematosus By Damage Cluster [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/identifying-phenotype-clusters-in-systemic-lupus-erythematosus-by-damage-cluster/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/identifying-phenotype-clusters-in-systemic-lupus-erythematosus-by-damage-cluster/