Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Low complement is associated with clinical disease activity and future organ damage in patients with systemic lupus erythematosus (SLE). Prior studies from Japan, although inconsistent, supported improvement in complement levels after hydroxychloroquine (HCQ) introduction. We studied HCQ whole blood levels and C3 and C4 levels in a US cohort.
Methods: In the first paired-visit analysis, to mimic the Japanese studies, we identified patients with low complement and low levels of HCQ in their blood.Then at their next clinic visit, we compared those whose HCQ whole blood levels increased to over 50 ng/mL to those whose HCQ whole blood levels did not with respect to changes in complement. In a second analysis, we considered all clinical visits in our cohort among patients who sometimes had low complement, and sometimes did not, and we examined the association between HCQ whole blood levels and low complement using conditional logistic regression.
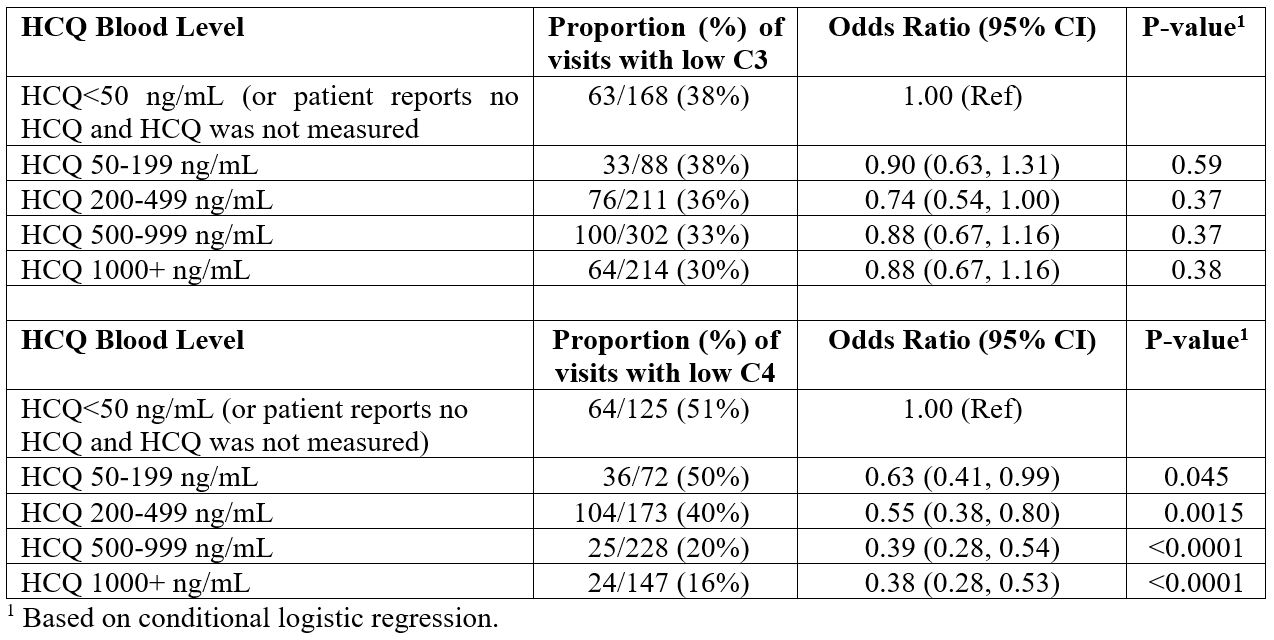
Results: Although the numbers varied between analyses, approximately 68% of the patients included in these analyses were African American, and 93% were female. Table 1 shows the results of the analysis of paired visits with respect to C3.Among those whose HCQ whole blood levels increased to be above 50 ng/mL, there was a greater mean increase in mean C3 (p=0.022) compared to those whose HCQ whole blood levels did not increase.Similarly, with respect to C4, among those HCQ whole blood levels increased, there was a significantly greater probability of achieving normal C4 levels (p=0.0030) and of having a higher increase in mean C4 (p=0.0037) (Table 2).Table 3 shows the results considering all clinic visits among those with variable complement levels. In this analysis, we did not observe a strong relationship between HCQ whole blood levels and C3. However, there was a consistently higher probability of achieving normal C4 levels as HCQ whole blood levels increased.
Conclusion: Both C3 and C4 levels increased significantly with HCQ whole blood levels >50 ng/mL. The percentage of patients who achieved a normal C4 level with a HCQ whole blood level >50 ng/mL (44%) was statistically significant. Surprisingly, even a low HCQ whole blood level was able to achieve an increase in complement. In the second analysis, we found a strong dose response between HCQ whole blood levels and C4 (but not C3). Improving complement levels may be one mechanism by which HCQ prevents poor outcomes in SLE. As low complement is part of the SLEDAI, this effect can contribute to an SRI-4 response in clinical trials.


To cite this abstract in AMA style:
Petri M, Jacobson R, Fava A, Magder L. Hydroxychloroquine Improves Low Complement Levels [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/hydroxychloroquine-improves-low-complement-levels/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/hydroxychloroquine-improves-low-complement-levels/