Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
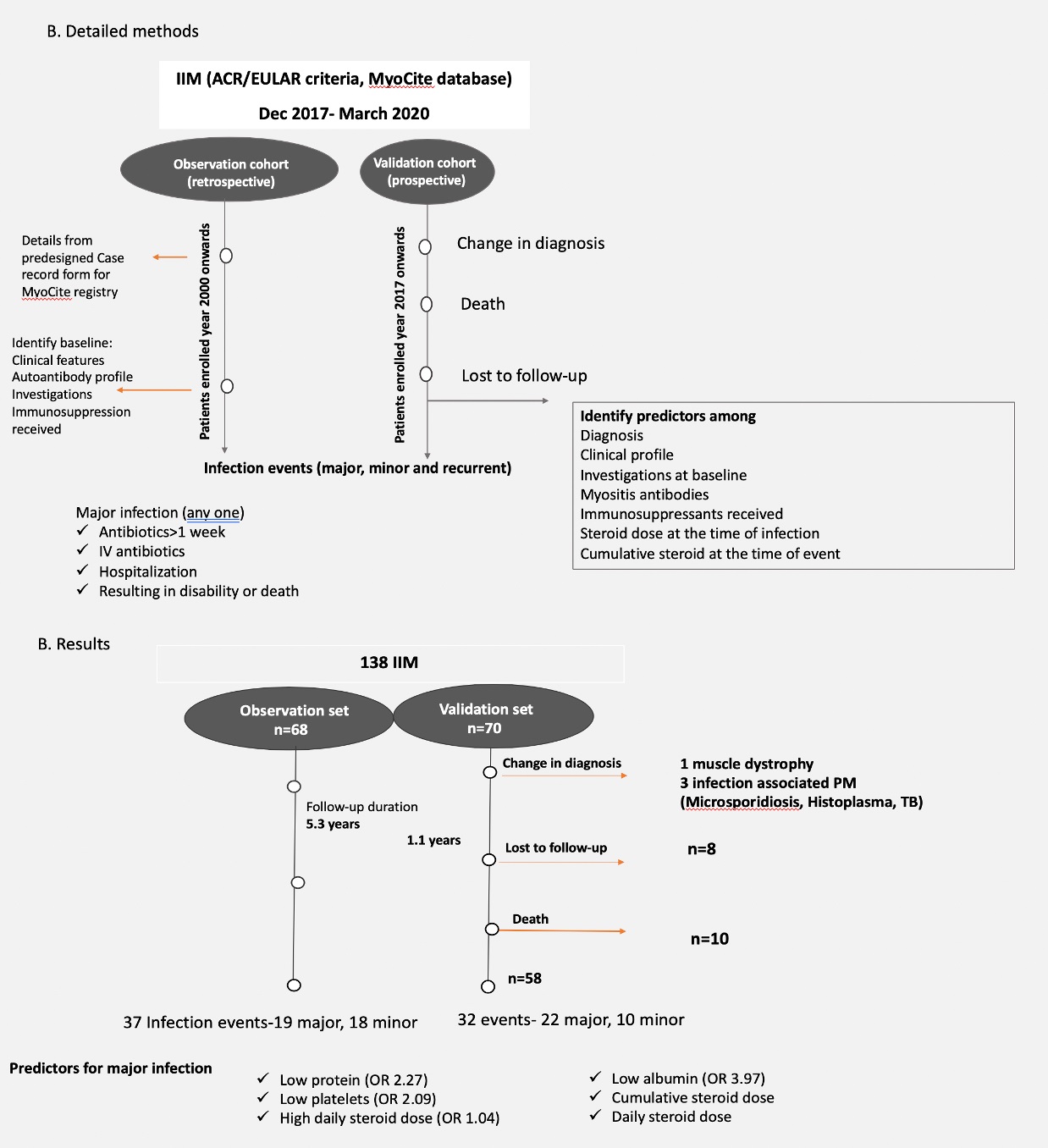
Background/Purpose: Infections are a major cause of morbidity and mortality in idiopathic inflammatory myopathy (IIM), more so in India.[1-3] The objective of this study was to characterize the profile and predictors of infections in IIM.
Methods: Details of IIM from the MyoCite database (Dec 2017- March 2020) were retrieved and characterised as the observation cohort.[4-6] The patients enrolled at inception during this period were followed up as the validation cohort to confirm findings from the observation cohort. Definitions and statistical analysis are detailed in Figure 1A. Descriptive data is expressed as median/mean (IQR/SD). Multivariate analysis was done using logistic regression. Missing values imputed using predictive means modelling. Statistical analysis was carried out on Rstudio version 1.2.5033.
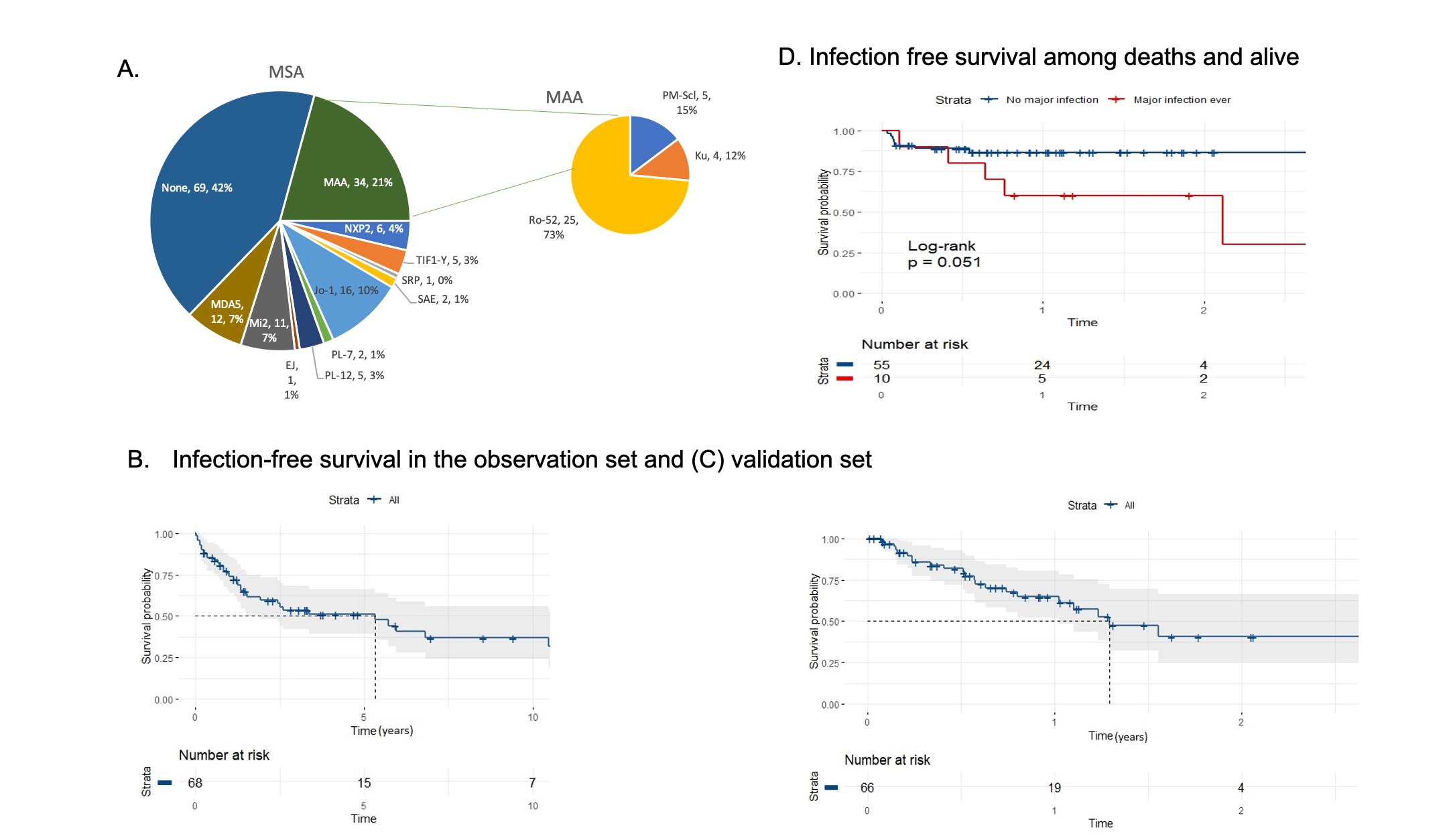
Results: A total 138 individuals (59 DM, 23 PM, 15 JDM, 34 OM, 3 CAM) were enrolled. Of these, 68 were in the retrospective observation cohort with median age 32 (25.5-42.4. F:M 4.2:1), and 66 prospectively enrolled at inception formed the validation cohort with median age 37 (21-47.7, F:M 3.7:1). Myositis antibodies are detailed in Figure 2 A.
Observation cohort.
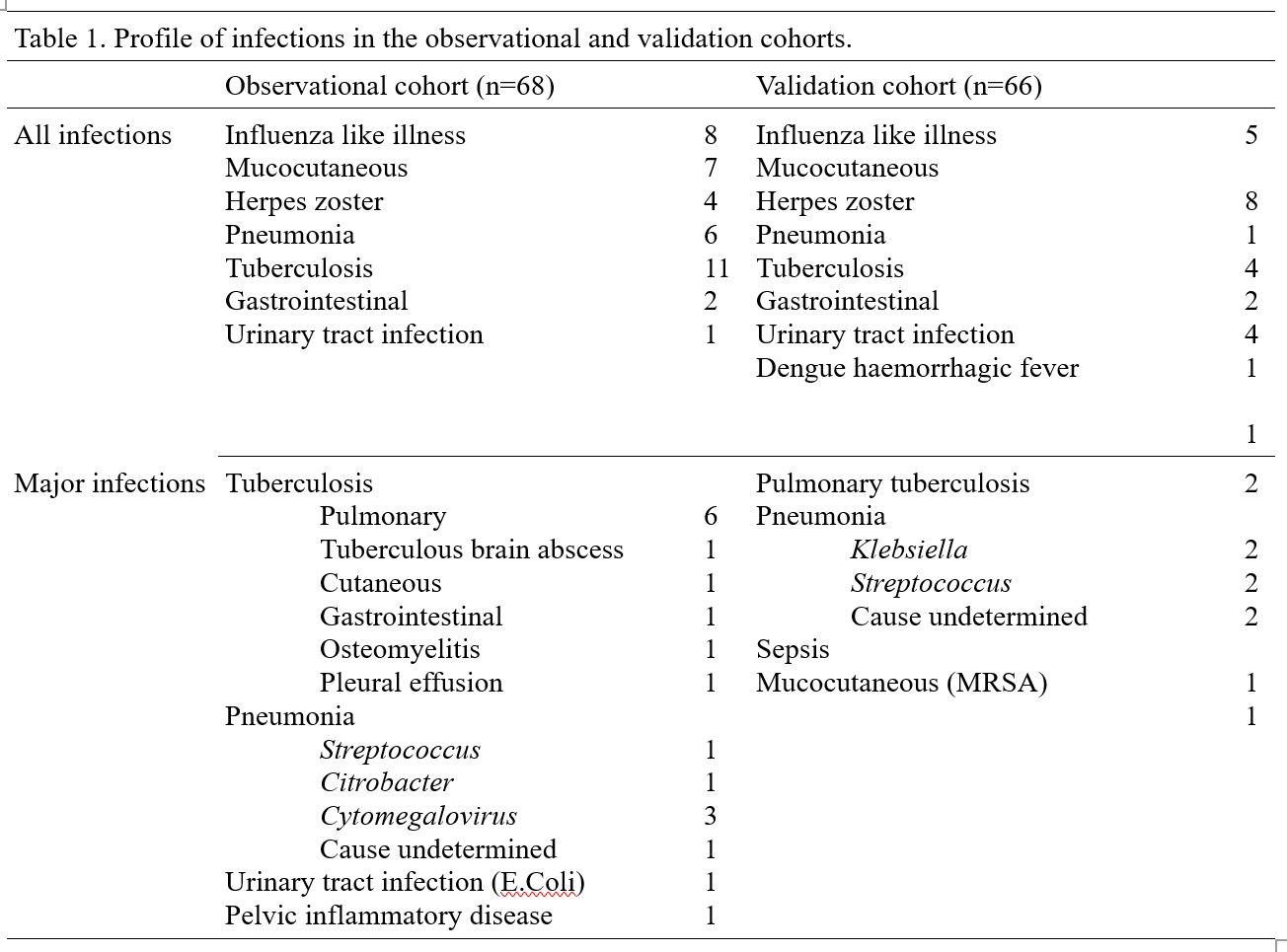
Over a mean follow up of 64 months, 37 patients had infections (Table 1), of which 19 (51.3%) were major. 11 (29%) had recurrent infections. Tuberculosis was the most common infection (29% of all infections; 57% of major infections), with 45% being extra-pulmonary. On multivariate logistic regression low protein (OR 2.27), low platelets (OR 2.09) and high daily steroid dose (OR 1.04) were predictors of major infections, with a model accuracy of 79%. Median infection free survival was 64.9 months (Figure 2B).
Validation cohort.
Over a mean follow up of 13.6 months, 4 patients were reclassified as non-IIM, of which 3 had atypical infections of the muscle tissue. Among those with IIM, 22 developed had infections, of which 10(45.4%) were major. Four (18%) had recurrent infections. Median infection free survival was 22.7 months. Mots common infection was community acquired pneumonia. On multivariate logistic regression, low albumin (OR 3.97) was a predictor of major infections, with a model accuracy of 90%.
There were 10 deaths, 1 of them as a direct result of infection. Any major infection in the disease course was associated with overall deaths (p=0.013, Figure 2D).
Conclusion: Infections are common and predispose to mortality in Indian patients with IIM. Tuberculosis is the leading case of infections in North India with a higher incidence of extrapulmonary forms, in early as well as established disease.
To cite this abstract in AMA style:
Chatterjee R, Mehta P, Agarwal V, Gupta L. High Burden of Infections in Indian Patients with Idiopathic Inflammatory Myopathy: Validation of Observations from the MyoCite Dataset [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/high-burden-of-infections-in-indian-patients-with-idiopathic-inflammatory-myopathy-validation-of-observations-from-the-myocite-dataset/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/high-burden-of-infections-in-indian-patients-with-idiopathic-inflammatory-myopathy-validation-of-observations-from-the-myocite-dataset/