Session Information
Date: Monday, November 9, 2015
Title: Vasculitis Poster II
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Title: Healthcare Utilization and Direct Medical
Costs of Giant Cell Arteritis
Background/Purpose: Giant cell arteritis (GCA) is the
most common systemic vasculitis in patients aged ≥ 50 years. Few studies
have evaluated the economic impact of this condition and have been limited to
inpatient-only data sources. Although the majority of healthcare for patients
with GCA is provided as an outpatient, utilization and costs from this
healthcare sector is largely unknown.
Methods: This study utilized a retrospective,
population-based cohort of patients diagnosed with GCA, as defined by 1990 ACR
criteria, in 1982-2009 and a reference cohort of patients without GCA matched
on age, sex, and calendar year from the same population. Standardized cost data
(inflation-adjusted to 2014 dollars) for 1987-2014 and outpatient utilization
data for 1995-2014 were obtained from the Mayo Clinic Cost Data Warehouse and
analyzed from one year before and up to five years after the GCA
diagnosis/index date. Utilization and costs were compared between GCA and
non-GCA cohorts using signed rank two-tailed paired analyses.
Results: The GCA cohort consisted of 147 patients
(118 female, 29 male) with a mean (±SD) age of 77.2 (±8.2). The non-GCA cohort
comprised 147 patients with a mean (±SD) age of 76.9 (±8.5) years.
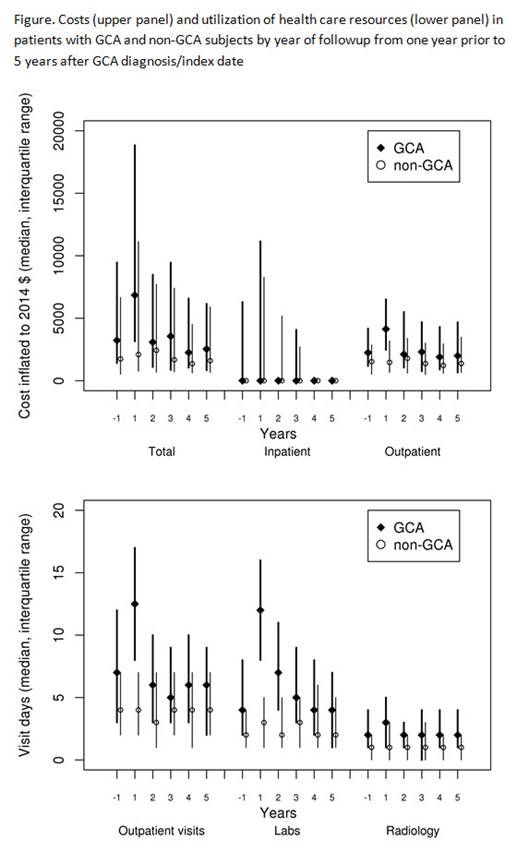
During the year preceding diagnosis, excess healthcare cost
related to GCA was only significantly increased in the month immediately
preceding GCA diagnosis [mean (±SD) excess cost $1127 (±5154)]. Following
diagnosis, significant annual excess outpatient cost was observed for patients
with GCA in each of the first four years [mean excess cost (±SD): 0-1 yrs $1307
(±15581), p<0.001; 1-2yrs $908 (±5917), p=0.009; 2-3 yrs $1324 (±4648),
p=0.007; 3-4 yrs $609 (±4596), p=0.04] but was similar between GCA and non-GCA
subjects in the 5th year. There were no significant differences in
inpatient costs between GCA and non-GCA subjects.
Patients with GCA had higher utilization of laboratory visit
days annually for each of the first 3 years following diagnosis, as well as
increased outpatient physician visits and combined radiology for years 0-1,
1-2, and 3-4 years (see figure). Ophthalmologic procedures/surgery were
increased for years 0-1, 1-2, and 4-5. Emergency medicine visits,
musculoskeletal and cardiovascular procedures/surgery were similar between GCA
and non-GCA groups throughout the study period.
Conclusion: Direct medical costs were increased in
the month preceding and outpatient costs were increased in the first 4 years
following GCA diagnosis and then return to levels similar to non-GCA subjects.
A higher utilization of outpatient physician, laboratory and radiology visits,
as well as ophthalmologic procedures among these patients accounts for the
observed increased cost of care.
To cite this abstract in AMA style:
Koster MJ, Achenbach SJ, Crowson CS, Matteson EL, Maradit Kremers H, Warrington KJ. Healthcare Utilization and Direct Medical Costs of Giant Cell Arteritis [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/healthcare-utilization-and-direct-medical-costs-of-giant-cell-arteritis/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/healthcare-utilization-and-direct-medical-costs-of-giant-cell-arteritis/