Session Information
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Early diagnosis and treatment of youth with SLE are crucial to prevent organ damage and reduce mortality. Understanding health care utilization prior to diagnosis may inform interventions to minimize diagnostic delay. We determined the frequency and associated factors for health care visits among youth with SLE in the year prior to diagnosis.
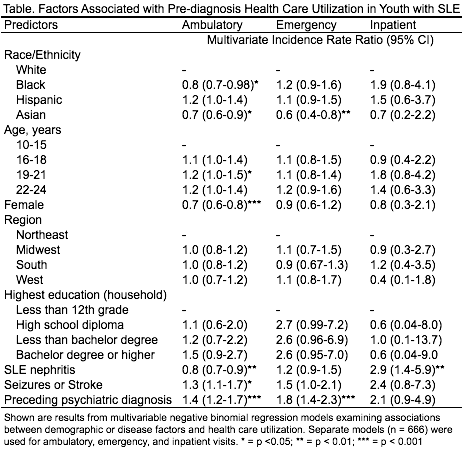
Methods: We used national administrative claims data (Optum Labs Data Warehouse) for privately insured U.S. enrollees from May 2000 to December 2013 to identify an incident cohort of youth ages 10-24 years with SLE. Incident cases were defined by ≥ 3 outpatient or inpatient visit claims with an ICD-9 primary diagnosis code for SLE (710.0) > 30 days apart, with ≥ 1 year of preceding continuous enrollment without a code for SLE. The mean number of ambulatory (AMB), emergency (ED), and inpatient (IP) visits in the year prior to the first SLE diagnosis code were compared to visits per year for healthy controls matched 2:1 by age and sex. For each SLE visit type, we also calculated the mean number of visits in the 3 and 6 months prior to diagnosis, and determined the most frequent primary diagnosis codes in the year prior. We used multivariable negative binomial regression models to examine associations between demographic or disease-related factors and AMB, ED, and IP utilization in the year prior to SLE diagnosis.
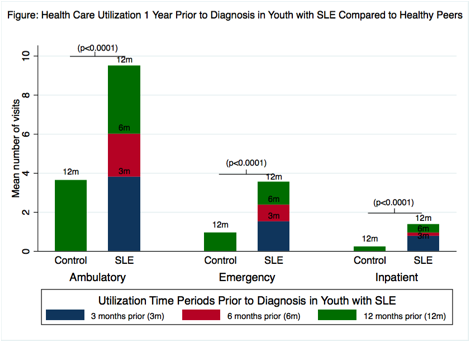
Results: We included 724 SLE subjects and 1448 controls comprised of 88% females, with a mean age of 18.6 years (standard deviation, SD 3.7). Compared to controls, fewer youth with SLE were white or from the Midwest; 24% had subsequent diagnoses for nephritis. Youth with SLE had significantly higher mean visits of all types in the year pre-diagnosis compared to controls: 9.5 (SD 10.0) vs 3.0 (4.5) for AMB (p<0.001), 3.6 (6.0) vs 0.9 (2.0) for ED (p <0.001), and 1.4 (4.4) vs 0.2 (1.5) for IP (p<0.001) (Figure). The most common primary diagnosis codes for pre-diagnosis AMB, ED and IP visits were: Other acne [706.1], Primary thrombocytopenia unspecified [287.3], and Fever unspecified [780.6], respectively. Subsequent nephritis was associated with decreased AMB, but increased IP visits. Preceding psychiatric diagnosis was associated with increased AMB and ED visits (Table). Female sex, Asian and Black race were associated with decreased AMB visits.
Conclusion: Youth with SLE have higher rates of health care utilization in the year preceding diagnosis compared to healthy peers. Strategies to improve early identification of youth with SLE, especially those presenting with psychiatric or renal manifestations, may allow earlier treatment and improve outcomes.
 |
To cite this abstract in AMA style:
Chang J, Brensinger C, Qing L, Knight A. Health Care Utilization Preceding Diagnosis of Systemic Lupus Erythematosus in Youth [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/health-care-utilization-preceding-diagnosis-of-systemic-lupus-erythematosus-in-youth/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/health-care-utilization-preceding-diagnosis-of-systemic-lupus-erythematosus-in-youth/