Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: New treatments have improved the short term outlook for patients with inflammatory polyarthritis (IP) over the past 20 years. However there is limited evidence on whether long term outcomes have changed. This study compared the 10 year outcomes (mortality, disease activity, disability) in 2 cohorts of patients recruited in 1990-4 and 2000-4.
Methods: Adults, aged ≥16 with ≥2 swollen joints for ≥4 weeks, were recruited to the Norfolk Arthritis Register (NOAR). Patients recruited from 1990-94 and 2000-04 made up cohorts 1 (C1) and 2 (C2) respectively. Patients were excluded if baseline assessment was ≥2 years after symptom onset. Baseline assessments included demographics, smoking status, 51 swollen / tender joint counts (SJC51 / TJC51), HAQ and self-report comorbidities. RF, ACPA and CRP were measured from stored blood samples. Patients were reassessed at 1-3, 5, 7 and 10 years. CRP was only measured at 5 and 10 years when blood samples were taken. Mortality data were provided by the Office for National Statistics. Censoring occurred after 10 years of follow up. The association between cohort and mortality was assessed using a Cox proportional hazard model. The associations between cohort and longitudinal disease activity (SJC51 / TJC51) / disability were assessed using random effects models. First age at symptom onset and gender were included as covariates. Then additional variables (baseline RF, ACPA, smoking status; time varying DMARD use, HAQ, SJC51, TJC51, CRP, comorbidities) were included.
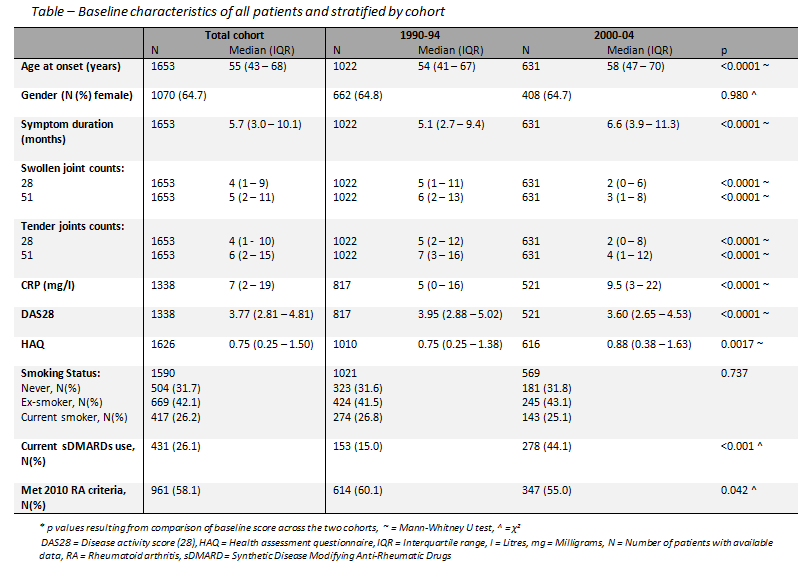
Results: Of 1653 included patients (C1 = 1022, C2 = 631), 962 (58.2%) patients met the 2010 RA criteria (C1 = 614 (60.1%), C2 = 348 (55.1%)). At baseline, patients in C2 were older, had lower SJC51 / TJC51 but had worse HAQ (see table). 948 patients (57.3%) completed 10 years of follow up (C1 = 607 (59.4%), C2 = 341 (54.0%)) whilst 306 (18.5%) patients died (C1 = 187 (18.3%), C2 = 119 (18.8%)). In an age and gender adjusted model, C2 was associated with a reduced risk of death compared to C1 (HR 0.77, 95% CI 0.61, 0.97). Adjusting further for possible confounders did not explain the reduced risk (HR 0.69, 95% CI 0.51, 0.94). C2 had lower longitudinal SJC51 compared to C1 in age and gender adjusted (SJC51: β -1.79, 95% CI -2.22, -1.36) and further adjusted models (SJC51: β -1.56 95% CI -1.94, -1.19). TJC51 was also lower in C2 and approached significance (age and gender adjusted: β -0.18, 95% CI -1.01, 0.65; further adjusted: β -0.65, 95% CI -1.31, 0.01). Physical disability was higher in C2 compared to C1 (β 0.09, 95% CI 0.03, 0.16), adjusting for age and gender. In the further adjusted model disability did not differ between cohorts (β -0.03, 95% CI -0.09, 0.03).
Conclusion: Over 10 years mortality risk and disease activity were improved in C2, although disability was not. C2 patients may have increased expectations of the efficacy of therapy or increased availability of devices may explain the similar HAQ scores.
To cite this abstract in AMA style:
Gwinnutt J, Symmons DPM, Macgregor AJ, Chipping J, Marshall T, Lunt M, Verstappen SMM. Have Outcomes of Patients with Inflammatory Arthritis Improved in the New Millennium? a Comparison of the 10 Year Outcome in Cohorts Recruited in 1990-4 and 2000-4 [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/have-outcomes-of-patients-with-inflammatory-arthritis-improved-in-the-new-millennium-a-comparison-of-the-10-year-outcome-in-cohorts-recruited-in-1990-4-and-2000-4/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/have-outcomes-of-patients-with-inflammatory-arthritis-improved-in-the-new-millennium-a-comparison-of-the-10-year-outcome-in-cohorts-recruited-in-1990-4-and-2000-4/