Session Information
Date: Saturday, November 7, 2020
Title: SLE – Treatment Poster I
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Systemic lupus erythematosus (SLE) patients are usually treated with glucocorticoids even during periods of clinically quiescent disease. A recent study showed that abrupt glucocorticoid withdrawal was associated with increased likelihood of flare in the next 12 months. The aim of the present study was to assess clinical flare rates and damage accrual in patients who tapered glucocorticoids gradually.
Methods: Lupus patients with two consecutive years of clinically quiescent disease were retrieved from our long-term longitudinal cohort. Individuals who maintained a low prednisone dose (5mg/day) comprised the maintenance group whereas patients who tapered prednisone within these two years comprised the withdrawal group. All individuals were followed for two years after discontinuation. Outcomes included clinical flares (any increase in clinical SLEDAI-2K, any increase ³4 and any increase in clinical SLEDAI-2K plus escalation in systemic therapy (glucocorticoids and/or antimalarials and/or immunosuppressives) as well as damage accrual. A Cox proportional regression analysis was performed for the identification of predictors for clinical flare.
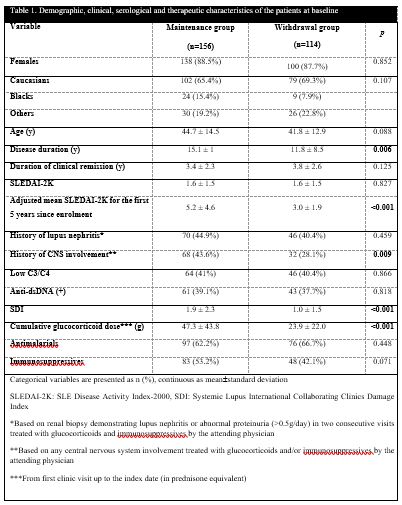
Results: Of 270 eligible patients, 156 maintained low dose prednisone and 114 discontinued gradually (62 within 12 months and 52 in 12-24 months). Demographic, clinical, serological and therapeutic characteristics are shown in Table 1. Patients in the withdrawal group developed significantly less flares by any applied definition at 24 months compared to the maintenance group, Table 2. Flare rates at 12 months were similarly better for withdrawal patients, although insignificantly. Regarding damage, less withdrawal patients accrued new damage at 24 months, Table 2. Further analysis of the slow (within 12-24 months) and fast (within 12 months) withdrawal patients demonstrated that the former group achieved better outcomes both for clinical flares and damage accrual, although insignificantly. Regarding predictors of flares, immunosuppressive therapy at baseline was associated with decreased likelihood of new flare [HR=0.64, 95%CI=0.435-0.943, p=0.024].
Conclusion: Gradual glucocorticoid withdrawal was associated with significantly less clinical flares at 24 months. Damage accrual was significantly less in the withdrawal patients. Immunosuppressive therapy at baseline was protective against new flares. Gradual glucocorticoid withdrawal is safe in clinically quiescent SLE.

To cite this abstract in AMA style:
Tselios K, Gladman D, Su J, Urowitz M. Gradual Glucocorticoid Withdrawal Is Safe in Clinically Quiescent Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/gradual-glucocorticoid-withdrawal-is-safe-in-clinically-quiescent-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/gradual-glucocorticoid-withdrawal-is-safe-in-clinically-quiescent-systemic-lupus-erythematosus/